"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="WxV_IOPE7-2309410982-linear-gradient" x1="1" x2="0" y1="0.5951279047551217" y2="0.4048720952448783"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="WwbAIQIz8-2309410982-linear-gradient" x1="0.43478742751482424" x2="0.6358595260107829" y1="0.26" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="ZWsVQcPfn-2309410982-linear-gradient" x1="0.9508213454678907" x2="0.04917865453210929" y1="0" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="lTyCGrzzP-2309410982-linear-gradient" x1="0.374937164194436" x2="0.625062835805564" y1="0" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient></defs><g d="M 658.002 1357.705 C 1020.321 1357.705 1314.04 1063.989 1314.04 701.667 C 1314.04 339.347 1020.321 45.626 658.002 45.626 C 295.681 45.626 1.96 339.347 1.96 701.667 L 0 701.667 C 0 338.263 294.598 43.665 658.002 43.665 C 1021.404 43.665 1316 338.263 1316 701.667 C 1316 1065.072 1021.404 1359.672 658.002 1359.672 C 294.598 1359.672 0 1065.072 0 701.667 L 1.96 701.667 C 1.96 1063.989 295.681 1357.705 658.002 1357.705 Z M 658.005 1265.053 C 969.154 1265.053 1221.392 1012.819 1221.392 701.667 C 1221.392 390.517 969.154 138.281 658.005 138.281 C 346.856 138.281 94.619 390.517 94.619 701.667 L 92.659 701.667 C 92.659 389.433 345.77 136.321 658.005 136.321 C 970.241 136.321 1223.352 389.433 1223.352 701.667 C 1223.352 1013.902 970.241 1267.017 658.005 1267.017 C 345.77 1267.017 92.659 1013.902 92.659 701.667 L 94.619 701.667 C 94.619 1012.819 346.856 1265.053 658.005 1265.053 Z M 658.002 1166.116 C 914.513 1166.116 1122.452 958.178 1122.452 701.667 C 1122.452 445.16 914.513 237.22 658.002 237.22 C 401.494 237.22 193.551 445.16 193.551 701.667 L 191.59 701.667 C 191.59 444.077 400.411 235.255 658.002 235.255 C 915.596 235.255 1124.412 444.077 1124.412 701.667 C 1124.412 959.261 915.596 1168.084 658.002 1168.084 C 400.411 1168.084 191.59 959.261 191.59 701.667 L 193.551 701.667 C 193.551 958.178 401.494 1166.116 658.002 1166.116 Z M 281.657 818.28 C 298.572 818.28 314.804 825.001 326.765 836.965 L 458.99 969.182 C 470.582 980.781 486.308 987.298 502.706 987.298 L 612.137 987.298 C 646.284 987.298 673.972 959.61 673.972 925.463 L 673.972 891.504 L 675.939 891.504 L 675.939 925.463 C 675.939 960.7 647.374 989.258 612.137 989.258 L 502.706 989.258 C 485.788 989.258 469.562 982.537 457.599 970.573 L 325.378 838.356 C 313.785 826.757 298.056 820.242 281.657 820.244 L 1.173 820.244 L 1.173 818.28 Z M 746.64 888.714 L 1053.046 888.714 C 1069.967 888.714 1086.194 895.435 1098.16 907.398 L 1259.381 1068.619 L 1257.99 1070.007 L 1096.772 908.79 C 1085.175 897.193 1069.446 890.679 1053.046 890.681 L 746.64 890.681 C 729.724 890.681 713.493 883.957 701.533 871.993 L 685.377 855.845 L 686.769 854.453 L 702.917 870.605 C 714.513 882.201 730.241 888.715 746.64 888.714 Z M 667.685 552 L 512.316 396.894 C 494.66 379.264 484.741 355.356 484.739 330.426 L 484.739 0 L 487.632 0 L 487.632 330.426 C 487.632 354.592 497.248 377.763 514.369 394.851 L 669.739 549.957 Z M 782.851 700.491 C 816.998 700.491 844.686 672.804 844.686 638.655 L 844.686 516.468 C 844.687 499.547 851.409 483.32 863.374 471.355 L 1177.508 157.22 L 1178.896 158.607 L 864.762 472.742 C 853.162 484.337 846.646 500.067 846.646 516.468 L 846.646 638.655 C 846.646 673.89 818.088 702.455 782.851 702.455 L 700.405 702.455 L 700.405 700.491 Z M 130.338 534.223 L 213.07 534.223 C 256.112 534.223 291.003 569.114 291.003 612.156 L 291.003 694.888 C 291.003 711.29 297.514 727.017 309.113 738.611 L 472.887 902.378 L 471.496 903.769 L 307.726 739.995 C 295.761 728.033 289.038 711.807 289.038 694.888 L 289.038 612.156 C 289.038 570.198 255.028 536.188 213.07 536.188 L 130.338 536.188 C 113.419 536.187 97.193 529.465 85.23 517.5 L 77.071 509.345 C 65.107 497.381 58.386 481.153 58.388 464.233 L 58.388 199.526 L 60.348 199.526 L 60.348 464.233 C 60.349 480.631 66.863 496.358 78.458 507.954 L 86.617 516.113 C 98.213 527.709 113.94 534.223 130.338 534.223 Z" fill="transparent" height="1359.6717183844698px" id="DcyumyANr" transform="translate(0 -43.665)" width="1316px"><g opacity="0.5"><path d="M 658.002 1314.039 C 1020.321 1314.039 1314.04 1020.324 1314.04 658.001 C 1314.04 295.681 1020.321 1.961 658.002 1.961 C 295.681 1.961 1.96 295.682 1.96 658.001 L 0 658.001 C 0 294.598 294.598 0 658.002 0 C 1021.404 0 1316 294.598 1316 658.001 C 1316 1021.407 1021.404 1316.007 658.002 1316.007 C 294.598 1316.007 0 1021.407 0 658.001 L 1.96 658.001 C 1.96 1020.324 295.681 1314.039 658.002 1314.039 Z" fill="rgb(255, 255, 255)" height="1316.0065114752902px" id="dxf13D52Y" transform="translate(0 43.665)" width="1316px"/></g><g opacity="0.3"><path d="M 565.347 1128.732 C 876.496 1128.732 1128.733 876.498 1128.733 565.346 C 1128.733 254.196 876.496 1.961 565.347 1.961 C 254.197 1.961 1.961 254.196 1.961 565.346 L 0 565.346 C 0 253.112 253.111 0 565.347 0 C 877.582 0 1130.693 253.112 1130.693 565.346 C 1130.693 877.581 877.582 1130.696 565.347 1130.696 C 253.111 1130.696 0 877.581 0 565.346 L 1.961 565.346 C 1.961 876.498 254.197 1128.732 565.347 1128.732 Z" fill="rgb(255, 255, 255)" height="1130.6960934794101px" id="if1BmYw1S" transform="translate(92.659 136.321)" width="1130.693351805604px"/></g><g opacity="0.15"><path d="M 466.412 930.861 C 722.923 930.861 930.862 722.922 930.862 466.411 C 930.862 209.905 722.923 1.965 466.412 1.965 C 209.904 1.965 1.961 209.905 1.961 466.411 L 0 466.411 C 0 208.822 208.821 0 466.412 0 C 724.006 0 932.822 208.822 932.822 466.411 C 932.822 724.005 724.006 932.828 466.412 932.828 C 208.821 932.828 0 724.005 0 466.411 L 1.961 466.411 C 1.961 722.922 209.904 930.861 466.412 930.861 Z" fill="rgb(255, 255, 255)" height="932.8284667407987px" id="ef75NsYf6" transform="translate(191.59 235.255)" width="932.8219552655086px"/></g><g opacity="0.5"><path d="M 280.484 0 C 297.399 0 313.63 6.721 325.592 18.685 L 457.817 150.902 C 469.408 162.501 485.135 169.018 501.533 169.017 L 610.964 169.017 C 645.111 169.017 672.799 141.33 672.799 107.182 L 672.799 73.223 L 674.766 73.223 L 674.766 107.182 C 674.766 142.42 646.201 170.978 610.964 170.978 L 501.533 170.978 C 484.614 170.978 468.389 164.257 456.426 152.293 L 324.205 20.076 C 312.611 8.477 296.883 1.961 280.484 1.964 L 0 1.964 L 0 0 Z" fill="url(%23cQ4xRdUtr-2309410982-linear-gradient)" height="170.97763275969464px" id="cQ4xRdUtr" transform="translate(1.173 818.28)" width="674.7656780356198px"/></g><g opacity="0.5"><path d="M 61.263 34.261 L 367.669 34.261 C 384.589 34.261 400.817 40.982 412.783 52.945 L 574.004 214.166 L 572.612 215.554 L 411.395 54.337 C 399.798 42.74 384.069 36.226 367.669 36.228 L 61.263 36.228 C 44.347 36.228 28.116 29.504 16.155 17.54 L 0 1.391 L 1.391 0 L 17.54 16.152 C 29.136 27.747 44.864 34.261 61.263 34.261 Z" fill="url(%23WxV_IOPE7-2309410982-linear-gradient)" height="215.55382175474415px" id="WxV_IOPE7" transform="translate(685.377 854.453)" width="574.0036823012563px"/></g><g opacity="0.5"><path d="M 182.946 552 L 27.577 396.894 C 9.921 379.264 0.002 355.356 0 330.426 L 0 0 L 2.893 0 L 2.893 330.426 C 2.893 354.592 12.509 377.763 29.63 394.851 L 185 549.957 Z" fill="url(%23WwbAIQIz8-2309410982-linear-gradient)" height="552px" id="WwbAIQIz8" transform="translate(484.739 0)" width="185px"/></g><g opacity="0.5"><path d="M 82.446 543.271 C 116.593 543.271 144.281 515.583 144.281 481.435 L 144.281 359.248 C 144.282 342.327 151.004 326.1 162.969 314.135 L 477.103 0 L 478.491 1.387 L 164.356 315.522 C 152.757 327.117 146.241 342.846 146.241 359.248 L 146.241 481.435 C 146.241 516.67 117.683 545.235 82.446 545.235 L 0 545.235 L 0 543.271 Z" fill="url(%23ZWsVQcPfn-2309410982-linear-gradient)" height="545.2346136318063px" id="ZWsVQcPfn" transform="translate(700.405 157.22)" width="478.4906210693257px"/></g><g opacity="0.5"><path d="M 71.95 334.696 L 154.682 334.696 C 197.724 334.696 232.616 369.588 232.616 412.63 L 232.616 495.362 C 232.616 511.764 239.126 527.491 250.725 539.084 L 414.5 702.851 L 413.108 704.243 L 249.338 540.469 C 237.373 528.507 230.651 512.281 230.651 495.362 L 230.651 412.63 C 230.651 370.672 196.64 336.661 154.682 336.661 L 71.95 336.661 C 55.031 336.661 38.805 329.939 26.843 317.974 L 18.683 309.819 C 6.719 297.854 -0.001 281.627 0 264.707 L 0 0 L 1.961 0 L 1.961 264.707 C 1.961 281.105 8.475 296.832 20.07 308.428 L 28.229 316.587 C 39.825 328.182 55.552 334.697 71.95 334.696 Z" fill="url(%23lTyCGrzzP-2309410982-linear-gradient)" height="704.2427839655832px" id="lTyCGrzzP" transform="translate(58.388 199.526)" width="414.49961191971533px"/></g></g></svg>)
The average physician spends more than 14 hours per week on prior authorization tasks [1]. That's nearly two full workdays spent not seeing patients, not documenting care, and not billing for services rendered.
It's spent on hold with payers, re-entering data that already exists in the EHR, and checking portal statuses that could change without notice.
Prior authorization was designed to ensure treatments are medically necessary and covered. The intent is reasonable. The execution is broken.
This guide covers how prior authorization automation works, which technologies power it, what the 2024 CMS Final Rule requires of your practice, and which platforms are leading the category.
Key Takeaway
Prior authorization automation uses AI, robotic process automation (RPA), and healthcare data standards like EDI X12 278 to automatically extract clinical data from EHR systems, submit PA requests to payers, and track approval status without manual staff intervention. The CAQH 2023 Index shows manual PA transactions cost providers approximately $11 per request compared to $2 for fully electronic transactions [3]. The 2024 CMS Interoperability and Prior Authorization Final Rule (effective January 2026) now requires payers to respond within 72 hours for urgent requests and seven days for standard requests, making automation not just a cost lever but a compliance necessity [2]. Platforms like Sully.ai go further by integrating PA automation into a coordinated AI workforce, where the AI Scribe captures documentation, the AI Coder extracts ICD-10 and CPT codes, and clean claims are submitted before denials occur.
Why Prior Authorization Creates a Bottleneck in Healthcare Delivery
Prior authorization is, at its core, a data problem. The clinical information payers need to make a decision already sits in the EHR. Getting it out, formatted correctly, and submitted to the right payer through the right channel is where things fall apart.
There are more than 1,000 payers in the US. Each has its own portal, its own forms, and its own criteria. Manual PA isn't just slow. It's structurally incapable of scaling.
The Administrative Cost of Manual PA Workflows
Each manual PA transaction costs a provider approximately $11.15, compared to $2.11 for a fully electronic transaction [3]. That gap adds up fast.
A practice submitting 50 PA requests per week spends more than $25,000 per year in transaction costs alone, before accounting for staff time. Add the time cost: the AMA's 2023 survey shows physicians spending 14-plus hours per week on PA tasks, and the total cost per request approaches $36 [1].
For every physician seeing patients, there are roughly 10 administrative staff behind them [1]. PA is a major reason why.
By the numbers: A practice with 200 PA requests per month could be spending more than $80,000 per year in combined transaction and staff time costs on prior authorization alone.
How PA Delays Affect Patient Outcomes
Speed matters in medicine. PA delays don't just frustrate staff. They harm patients.
According to AMA data, 93% of physicians say PA delays patient care [1]. More troubling: 25% report that a PA delay led to a serious adverse event for a patient, including hospitalization or permanent damage [1].
When a patient is waiting on approval for a specialty medication, they're often managing a chronic condition that gets worse without treatment. If approval takes five days and the patient stops their regimen in the meantime, both the outcome and the downstream billing opportunity suffer.
Staff Burnout Driven by High-Volume PA Tasks
PA is exactly the kind of work that burns people out: repetitive, rules-based, high-volume, and consequential if you get it wrong.
Staff spend hours on hold with payer call centers, re-entering data that already exists in the chart, and logging into multiple portals to track submissions. This isn't a small-practice problem. Health systems running Epic still have dedicated PA teams navigating payer portals by hand.
Automation exists to eliminate this kind of work. PA is near the top of the list.
How Prior Authorization Automation Works
Modern PA automation isn't a form-filler or a portal shortcut. It's a system that reads clinical data, applies payer rules, submits the request through the right channel, and tracks the response, all without a staff member touching it [4].
Here's how each step works in practice.
AI-Driven Data Extraction from EHR Systems
When a provider orders a procedure or medication that requires PA, the system reads the patient's chart automatically. It pulls diagnosis codes, lab values, medication history, and prior treatment records.
This is where natural language processing (NLP) makes a real difference. AI can extract data from unstructured physician notes, not just structured EHR fields. If a note says the patient tried and failed two prior medications, the system captures that without anyone reading and re-typing it [4].
The manual alternative: a staff member opens the EHR, reads the chart, then manually re-enters values into a payer portal. Automation eliminates that entire step.
Automated Submission Through EDI 278 and Payer Portals
Once the data is assembled, the system submits the PA request through the appropriate channel. There are three main options:
EDI X12 278 (the HIPAA-mandated standard for PA requests and responses)
Payer APIs (increasingly available as FHIR requirements expand)
RPA-driven portal automation (for payers that still don't offer API access)
The system selects the right channel based on payer and plan type. As CMS requirements push more payers to support FHIR APIs by January 2026, the mix will shift further toward real-time API submission and away from portal workarounds [2].
Real-Time Status Tracking Without Staff Intervention
After submission, the system polls for responses automatically. No one needs to call the payer or check a portal.
When the payer responds (approved, denied, or requesting additional information), the system routes the decision back into the EHR and notifies the right team member. Denials can automatically trigger appeal workflows with supporting documentation pre-populated.
This step alone eliminates several hours of follow-up work per staff member per week.
Technologies Powering Prior Authorization Automation
PA automation isn't one technology. It's a stack. Understanding what each layer does helps when evaluating vendors, because not every platform uses all of them [4].
Robotic Process Automation in PA Workflows
RPA uses software bots to mimic human actions in web interfaces: logging into payer portals, navigating forms, clicking buttons, and downloading decisions.
It was the first major PA automation technology and is still widely used because most payers don't offer API access. The limitation is real, though. RPA is brittle. It breaks when a payer changes its portal UI, and it doesn't understand clinical context. It automates mechanical steps but not judgment calls.
RPA works best as a stopgap for payers without EDI or FHIR API support, not as a long-term foundation.
AI and Natural Language Processing for Clinical Data
AI and NLP add the intelligence layer that RPA lacks. They can read a physician's note and identify that a patient tried and failed two prior medications, a common payer requirement for approving a specialty drug.
They can also flag missing documentation before the PA goes out. That pre-submission validation is where the denial-rate impact comes from. Generative AI is now being applied here too: some platforms can draft prior authorization letters and clinical justifications directly from patient data [4].
MACPAC has documented that AI adoption in Medicaid PA contexts is accelerating, with more programs moving toward AI-assisted automation rather than pure RPA [4].
Healthcare APIs and EDI Standards
EDI X12 278 is the HIPAA-mandated standard for PA requests and responses. Adoption has been uneven. Many payers still route PA through portals rather than EDI, which is why RPA remains in the picture.
HL7 FHIR APIs represent the next generation. The CMS 2024 Final Rule requires Medicare Advantage, Medicaid, and CHIP payers to support FHIR-based PA APIs by January 2026, enabling real-time data exchange [2]. Three key FHIR implementation guides govern PA: CRD (Coverage Requirements Discovery), DTR (Documentation Templates and Rules), and PAS (Prior Authorization Support).
If you're evaluating a PA automation vendor, ask which of these they support. The answer tells you a lot about their technical roadmap.
What the CMS Prior Authorization Final Rule Means for Providers
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), finalized in January 2024, is the most significant federal action on PA in decades. Most coverage focuses on what payers must do. The provider implications matter just as much [2].
New Decision Timelines and Compliance Requirements
Starting January 1, 2026, Medicare Advantage, Medicaid, and CHIP plans must meet new requirements across the board.
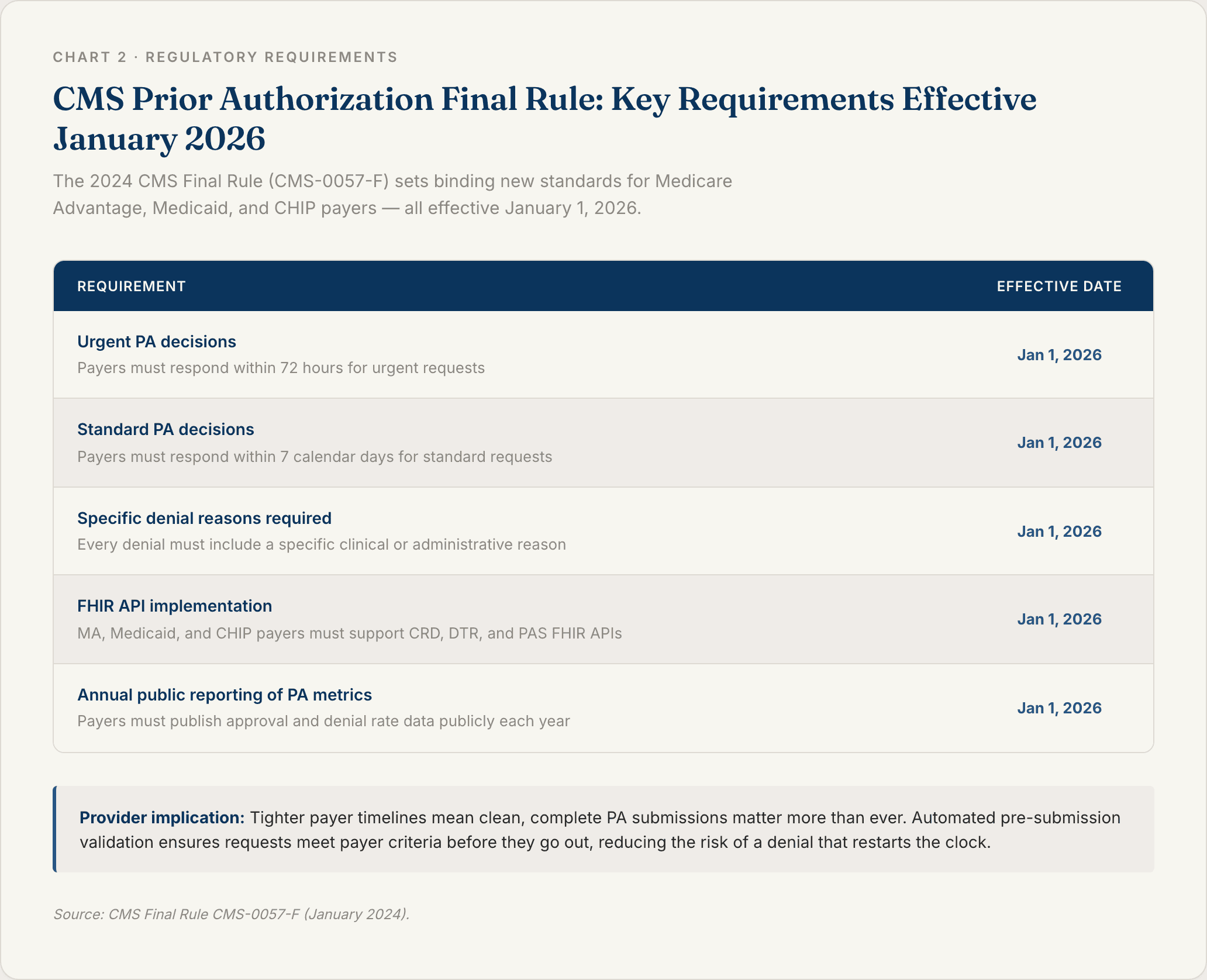
The requirement that payers provide a specific reason for every denial is particularly significant. It gives providers a clear basis for appeal, and it gives automation platforms real data to improve pre-submission validation over time.
For providers, tighter payer timelines create pressure to submit complete, well-documented requests on the first pass. Automated systems that pre-validate against payer criteria before submission dramatically reduce the risk of a denial that restarts the clock.
FHIR API Standards and EHR Integration
The rule also requires covered payers to implement FHIR APIs using the CRD, DTR, and PAS implementation guides by January 2026. For providers, this creates a real opportunity [2].
If your PA automation platform supports FHIR, you can request PA determinations in real time at the point of care, before the patient leaves the office. That closes the gap between ordering a treatment and knowing whether it's covered.
Epic and Cerner are both building FHIR PA workflows into their platforms. Providers evaluating PA automation should verify whether their vendor is certified against the CMS IG specifications. That compatibility is what enables real-time PA at the point of prescribing.
The Business Case for Prior Authorization Software
The ROI of PA automation comes from two places: reducing what you spend per transaction, and reducing how often you need to rework a denial. Both add up faster than most finance teams expect [1][3].
Prior Authorization Best Practices That Reduce Denial Rates
The biggest driver of PA ROI isn't speed. It's denial prevention.
First-pass PA denial rates at many practices exceed 30% [5][6]. Every denial triggers rework: additional documentation, appeal letters, resubmission. That rework costs money and delays care further.
Automation reduces denial rates through four mechanisms:
Pre-submission criteria matching: The system checks the patient record against payer criteria before sending, so only complete, qualifying requests go out.
Clinical documentation alerts: If a required element is missing (like documentation of a failed first-line therapy), the system flags it before submission.
Payer-specific rule libraries: Platforms that maintain current payer criteria databases mean the system knows what each payer requires, updated continuously.
Appeal automation: When a denial comes in, the system routes it to the appropriate appeal workflow with supporting documentation already populated.
Automation that applies pre-submission validation can bring first-pass denial rates below 5% for many procedure types [3].
ROI and Cost Savings Compared to Manual Prior Authorization Workflows
Here's a model you can apply to your own practice:
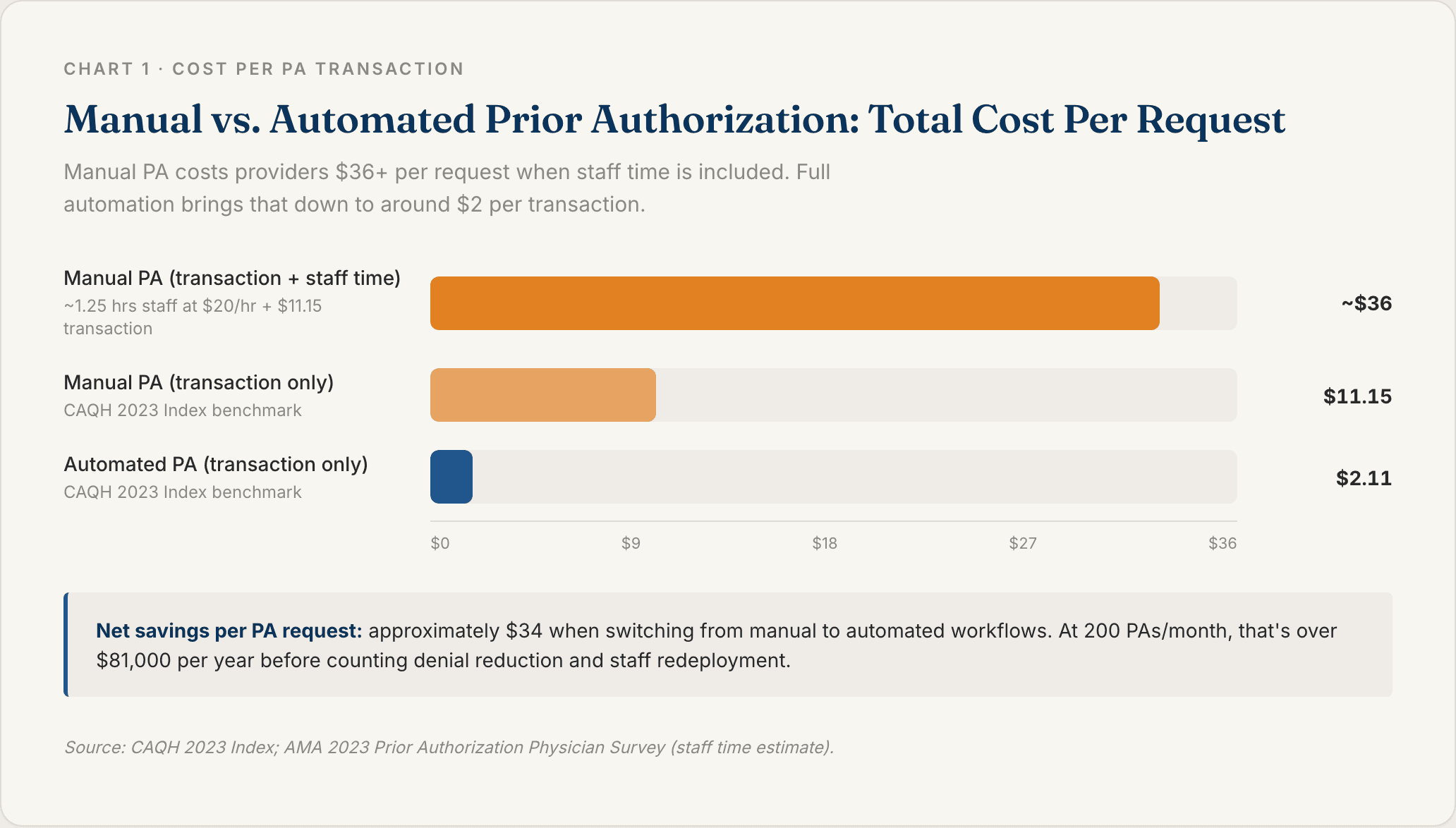
Manual PA: approximately $11.15 per transaction (CAQH) plus roughly $25 in staff time at an estimated 1.25 hours per request [1][3]
Automated PA: approximately $2.11 per transaction plus near-zero staff time for standard cases
Net savings per PA: approximately $34
At 200 PAs per month: around $6,800 per month, or $81,600 per year
That's before counting indirect savings from fewer denied claims, fewer appeals, fewer write-offs, and recaptured staff time for higher-value work.
Sully.ai's AI roles cost 80-90% less than human equivalents. For practices running dedicated PA coordinator headcount, the math shifts dramatically once automation handles the volume.
Faster Time to Therapy and Patient Satisfaction
In value-based care models, patient experience affects reimbursement. When PA is delayed, patients miss appointments, abandon prescriptions, or switch providers.
Automated PA can compress the approval cycle from three to five days down to same-day or next-day for many standard requests. For specialty medications, that difference means patients start therapy faster, which improves medication adherence, outcomes, and quality scores like STAR ratings.
Better PA speed is better clinical performance. The two are directly connected.
Prior Authorization Automation Platforms Worth Evaluating
Not all PA automation platforms work the same way. Some focus exclusively on PA. Others embed it within a broader administrative workflow. Here's how the leading options compare.
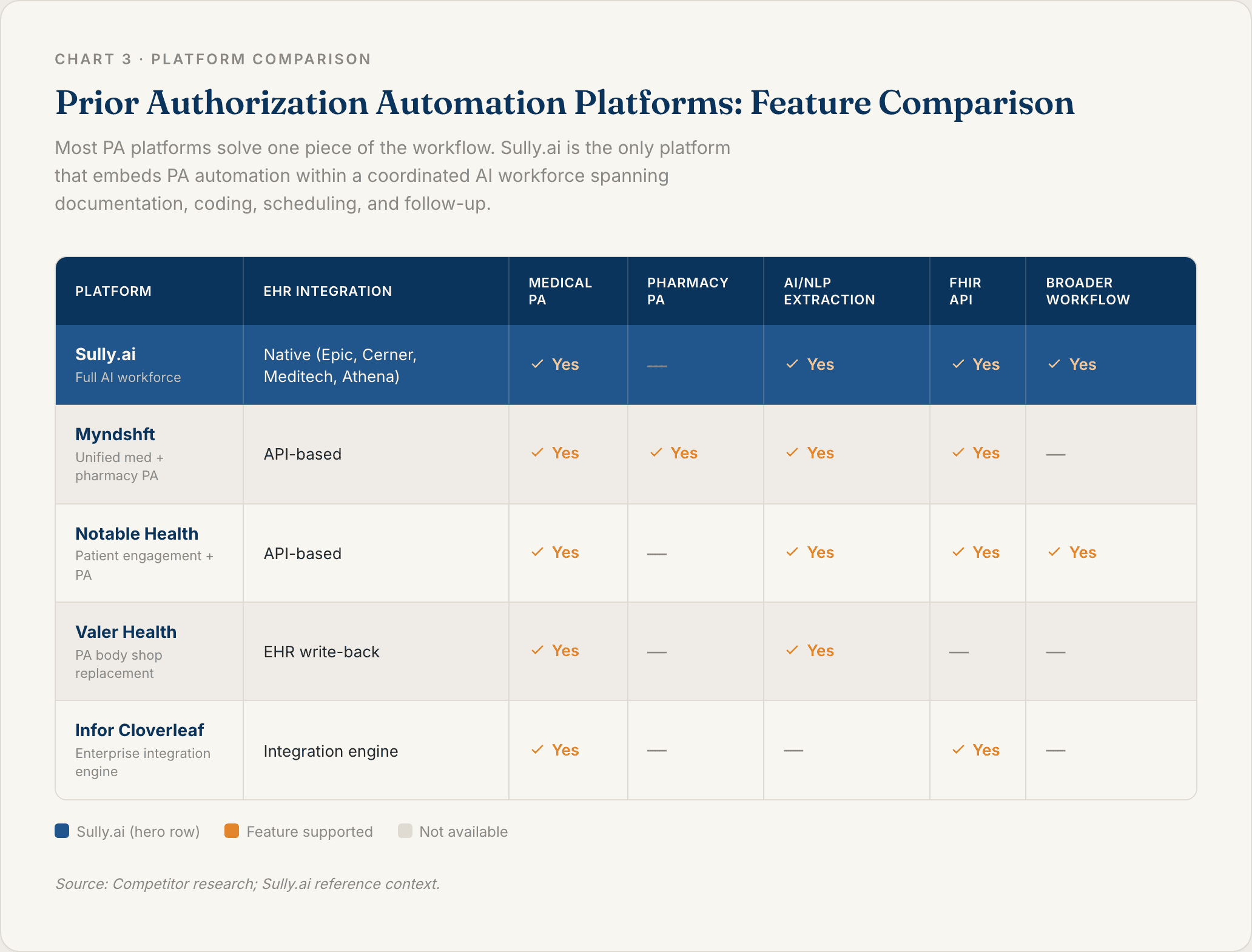
1. Sully.ai
Sully.ai approaches prior authorization differently from every other platform on this list. Rather than offering a standalone PA tool, Sully deploys a coordinated AI workforce where PA automation is built into the clinical and billing workflow from the start.
The AI Scribe captures the clinical encounter. The AI Coder extracts every ICD-10 and CPT code from the documentation. The system identifies whether the ordered procedure or medication requires PA, assembles the request with clinical documentation already in hand, and submits the clean claim before a denial can occur. No separate portal. No manual handoff. No siloed tool to manage on top of everything else.
Sully integrates once with the EHR (Epic, Cerner, Meditech, Athenahealth) and all agents share context. Operates 24/7 at 80-90% less cost than the human roles they replace.
2. Myndshft
Myndshft is the only platform in this category to offer unified medical and pharmacy PA automation on a single platform. It uses a self-learning rules engine with a synchronized payer criteria library, enabling real-time PA determinations for both medication and procedure requests.
Best fit for organizations that need to manage medical and pharmacy PA at scale, including health systems and payers looking for shared infrastructure.
3. Notable Health
Notable Health builds PA automation as part of a broader AI-driven patient engagement and workflow platform. Its PA workflow follows five stages: criteria detection, data collection, request submission, status tracking, and denial management, all agent-driven without staff involvement.
Strong for health systems that want PA automation embedded within a larger clinical workflow initiative rather than managed as a separate product.
4. Valer Health
Valer targets one specific problem: replacing the manual PA body shop. Most large practices run dedicated PA teams that still review, confirm, and submit each request by hand. Valer's platform handles submission, status tracking, payer decision verification, and EHR write-back automatically, with minimal human touchpoints.
Worth evaluating if your practice still runs a PA coordinator team and you want a direct replacement for that headcount.
5. Infor Cloverleaf
Infor Cloverleaf approaches PA from an integration engine perspective. It uses cloud-based microservices and event-driven workflows to standardize PA submissions and responses across complex health system environments.
Best suited for enterprise health systems already running Cloverleaf for clinical data integration that want to extend that infrastructure to cover PA workflows.
Prior Authorization Automation as Part of an AI-Driven Healthcare Workforce
PA automation as a standalone tool solves one problem. It doesn't fix the data fragmentation, the documentation burden, or the post-visit follow-up gap that sit on either side of it.
The practices seeing the biggest gains aren't just automating PA. They're connecting it to the full administrative workflow.
From Clinical Documentation to Clean Claim Without Manual Touchpoints
Here's what an end-to-end automated PA workflow looks like when documentation and coding are part of the same system:
The AI Scribe captures the clinical encounter in real time during the visit
The AI Coder extracts every ICD-10 and CPT code from the documentation
The system identifies whether the ordered procedure or medication requires PA
The PA request is assembled and submitted automatically, with clinical documentation already in hand
The clean claim is submitted before a denial can occur
PA platforms that sit outside the documentation workflow have to re-extract data the EHR already contains. That re-extraction step is where errors get introduced and time gets wasted.
Sully eliminates that step because the Scribe and Coder operate on the same patient record, in real time, as part of the same system. The clinical data flows directly into the PA request without anyone touching it in between.
How AI Agents Collaborate Across the Full Revenue Cycle
The coordination doesn't stop at PA submission. After PA is approved, the AI Receptionist confirms the appointment. After the visit, the AI Triage Nurse follows up on prescription adherence. If a patient hasn't filled their prescription, the Nurse reaches out. If they don't respond, the Receptionist books the follow-up slot.
No patient falls through. No manual follow-up call needed.
Sully operates across 5,000-plus providers and has delivered more than 50 million hours of AI work. That's what separates a workforce from a toolset: agents that share context, hand off cases, and operate as a team rather than as separate products.
If your practice is ready to stop managing PA as a standalone problem and start treating it as one layer of a coordinated administrative system, request a demo at sully.ai.
FAQ
Q: What is prior authorization automation?
Prior authorization automation uses AI, RPA, and healthcare data standards (EDI X12 278, FHIR APIs) to handle PA requests without manual staff intervention. Instead of a staff member logging into a payer portal, extracting data from the EHR, and typing it into a form, an automated system extracts the clinical data, matches it against payer criteria, submits the request, and tracks the response. Platforms like Sully.ai go further, connecting PA automation to clinical documentation and coding so clean claims are submitted before denials occur.
Q: How does prior authorization automation integrate with EHR systems?
Most PA automation platforms integrate with EHR systems via HL7 FHIR APIs, HL7 v2 interfaces, or native EHR app store integrations (Epic App Orchard, Cerner App Market). The integration lets the automation platform read patient charts, pull diagnostic codes and clinical documentation, and write PA status back into the patient record. Sully.ai uses a single EHR integration that works across Epic, Cerner, Meditech, and Athenahealth, so all AI agents (including the AI Coder that handles PA-adjacent billing tasks) share the same patient data without duplicate integrations.
Q: What is the CMS Interoperability and Prior Authorization Final Rule?
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), finalized in January 2024, requires Medicare Advantage, Medicaid, and CHIP payers to implement FHIR-based PA APIs by January 1, 2026 and to respond to standard PA requests within seven calendar days and urgent requests within 72 hours [2]. Payers must also provide specific reasons for all denials and report PA metrics publicly. For providers, this rule accelerates the shift toward real-time, EHR-embedded PA, making now the right time to evaluate platforms that support FHIR-based workflows.
Q: How does prior authorization automation reduce claim denials?
Automated PA systems apply pre-submission validation: checking the PA request against payer-specific criteria before it's sent. Requests missing required documentation, failing payer criteria, or routed to the wrong channel are caught before submission, not after. First-pass denial rates from manual PA often exceed 30% [5][6]. Automated systems with payer rules libraries and clinical data extraction can bring that figure below 5% for many procedure types, reducing the cost of appeals and the revenue lost from abandoned claims [3].
Q: What is the best prior authorization automation software for healthcare providers?
The best platform depends on your practice's scope. Sully.ai is best for organizations that want PA automation as part of a coordinated AI workforce, connecting documentation, coding, PA, and follow-up in a single integrated system. Myndshft is best for organizations managing both medical and pharmacy PA at scale. Notable Health is strong for health systems embedding PA automation within broader patient engagement workflows. Valer Health is a good fit for practices with dedicated PA teams that need a direct replacement for manual workflows. Infor Cloverleaf suits enterprise health systems with complex integration environments.
Sources
[1] American Medical Association (AMA) — 2023 AMA Prior Authorization Physician Survey. https://www.ama-assn.org/practice-management/prior-authorization/2023-ama-prior-authorization-survey-results
[2] Centers for Medicare & Medicaid Services (CMS) — CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F). https://www.cms.gov/newsroom/fact-sheets/cms-interoperability-and-prior-authorization-final-rule-cms-0057-f-0
[3] CAQH — 2023 CAQH Index: A Report on the Adoption of Electronic Business Transactions. https://www.caqh.org/explorations/caqh-index
[4] MACPAC (Medicaid and CHIP Payment and Access Commission) — Automation in the Prior Authorization Process. https://www.macpac.gov/publication/automation-in-the-prior-authorization-process/
[5] KFF (Kaiser Family Foundation) — Prior Authorization in Medicare Advantage. https://www.kff.org/medicare/issue-brief/prior-authorization-in-medicare-advantage/
[6] HHS Office of Inspector General (OIG) — Some Medicare Advantage Organization Denials of Prior Authorization Requests Raise Concerns About Beneficiary Access to Medically Necessary Care. https://oig.hhs.gov/reports-and-publications/featured-reports/medicare-advantage-prior-authorization/
TABLE OF CONTENTS
Hire your
Medical AI Team
Take a look at our Medical AI Team
AI Receptionist
Manages patient scheduling, communications, and front-desk operations across all channels.
AI Scribe
Documents clinical encounters and maintains accurate EHR/EMR records in real-time.
AI Medical Coder
Assigns and validates medical codes to ensure accurate billing and regulatory compliance.
AI Nurse
Assesses patient urgency and coordinates appropriate care pathways based on clinical needs.