"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="WxV_IOPE7-2309410982-linear-gradient" x1="1" x2="0" y1="0.5951279047551217" y2="0.4048720952448783"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="WwbAIQIz8-2309410982-linear-gradient" x1="0.43478742751482424" x2="0.6358595260107829" y1="0.26" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="ZWsVQcPfn-2309410982-linear-gradient" x1="0.9508213454678907" x2="0.04917865453210929" y1="0" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="lTyCGrzzP-2309410982-linear-gradient" x1="0.374937164194436" x2="0.625062835805564" y1="0" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient></defs><g d="M 658.002 1357.705 C 1020.321 1357.705 1314.04 1063.989 1314.04 701.667 C 1314.04 339.347 1020.321 45.626 658.002 45.626 C 295.681 45.626 1.96 339.347 1.96 701.667 L 0 701.667 C 0 338.263 294.598 43.665 658.002 43.665 C 1021.404 43.665 1316 338.263 1316 701.667 C 1316 1065.072 1021.404 1359.672 658.002 1359.672 C 294.598 1359.672 0 1065.072 0 701.667 L 1.96 701.667 C 1.96 1063.989 295.681 1357.705 658.002 1357.705 Z M 658.005 1265.053 C 969.154 1265.053 1221.392 1012.819 1221.392 701.667 C 1221.392 390.517 969.154 138.281 658.005 138.281 C 346.856 138.281 94.619 390.517 94.619 701.667 L 92.659 701.667 C 92.659 389.433 345.77 136.321 658.005 136.321 C 970.241 136.321 1223.352 389.433 1223.352 701.667 C 1223.352 1013.902 970.241 1267.017 658.005 1267.017 C 345.77 1267.017 92.659 1013.902 92.659 701.667 L 94.619 701.667 C 94.619 1012.819 346.856 1265.053 658.005 1265.053 Z M 658.002 1166.116 C 914.513 1166.116 1122.452 958.178 1122.452 701.667 C 1122.452 445.16 914.513 237.22 658.002 237.22 C 401.494 237.22 193.551 445.16 193.551 701.667 L 191.59 701.667 C 191.59 444.077 400.411 235.255 658.002 235.255 C 915.596 235.255 1124.412 444.077 1124.412 701.667 C 1124.412 959.261 915.596 1168.084 658.002 1168.084 C 400.411 1168.084 191.59 959.261 191.59 701.667 L 193.551 701.667 C 193.551 958.178 401.494 1166.116 658.002 1166.116 Z M 281.657 818.28 C 298.572 818.28 314.804 825.001 326.765 836.965 L 458.99 969.182 C 470.582 980.781 486.308 987.298 502.706 987.298 L 612.137 987.298 C 646.284 987.298 673.972 959.61 673.972 925.463 L 673.972 891.504 L 675.939 891.504 L 675.939 925.463 C 675.939 960.7 647.374 989.258 612.137 989.258 L 502.706 989.258 C 485.788 989.258 469.562 982.537 457.599 970.573 L 325.378 838.356 C 313.785 826.757 298.056 820.242 281.657 820.244 L 1.173 820.244 L 1.173 818.28 Z M 746.64 888.714 L 1053.046 888.714 C 1069.967 888.714 1086.194 895.435 1098.16 907.398 L 1259.381 1068.619 L 1257.99 1070.007 L 1096.772 908.79 C 1085.175 897.193 1069.446 890.679 1053.046 890.681 L 746.64 890.681 C 729.724 890.681 713.493 883.957 701.533 871.993 L 685.377 855.845 L 686.769 854.453 L 702.917 870.605 C 714.513 882.201 730.241 888.715 746.64 888.714 Z M 667.685 552 L 512.316 396.894 C 494.66 379.264 484.741 355.356 484.739 330.426 L 484.739 0 L 487.632 0 L 487.632 330.426 C 487.632 354.592 497.248 377.763 514.369 394.851 L 669.739 549.957 Z M 782.851 700.491 C 816.998 700.491 844.686 672.804 844.686 638.655 L 844.686 516.468 C 844.687 499.547 851.409 483.32 863.374 471.355 L 1177.508 157.22 L 1178.896 158.607 L 864.762 472.742 C 853.162 484.337 846.646 500.067 846.646 516.468 L 846.646 638.655 C 846.646 673.89 818.088 702.455 782.851 702.455 L 700.405 702.455 L 700.405 700.491 Z M 130.338 534.223 L 213.07 534.223 C 256.112 534.223 291.003 569.114 291.003 612.156 L 291.003 694.888 C 291.003 711.29 297.514 727.017 309.113 738.611 L 472.887 902.378 L 471.496 903.769 L 307.726 739.995 C 295.761 728.033 289.038 711.807 289.038 694.888 L 289.038 612.156 C 289.038 570.198 255.028 536.188 213.07 536.188 L 130.338 536.188 C 113.419 536.187 97.193 529.465 85.23 517.5 L 77.071 509.345 C 65.107 497.381 58.386 481.153 58.388 464.233 L 58.388 199.526 L 60.348 199.526 L 60.348 464.233 C 60.349 480.631 66.863 496.358 78.458 507.954 L 86.617 516.113 C 98.213 527.709 113.94 534.223 130.338 534.223 Z" fill="transparent" height="1359.6717183844698px" id="DcyumyANr" transform="translate(0 -43.665)" width="1316px"><g opacity="0.5"><path d="M 658.002 1314.039 C 1020.321 1314.039 1314.04 1020.324 1314.04 658.001 C 1314.04 295.681 1020.321 1.961 658.002 1.961 C 295.681 1.961 1.96 295.682 1.96 658.001 L 0 658.001 C 0 294.598 294.598 0 658.002 0 C 1021.404 0 1316 294.598 1316 658.001 C 1316 1021.407 1021.404 1316.007 658.002 1316.007 C 294.598 1316.007 0 1021.407 0 658.001 L 1.96 658.001 C 1.96 1020.324 295.681 1314.039 658.002 1314.039 Z" fill="rgb(255, 255, 255)" height="1316.0065114752902px" id="dxf13D52Y" transform="translate(0 43.665)" width="1316px"/></g><g opacity="0.3"><path d="M 565.347 1128.732 C 876.496 1128.732 1128.733 876.498 1128.733 565.346 C 1128.733 254.196 876.496 1.961 565.347 1.961 C 254.197 1.961 1.961 254.196 1.961 565.346 L 0 565.346 C 0 253.112 253.111 0 565.347 0 C 877.582 0 1130.693 253.112 1130.693 565.346 C 1130.693 877.581 877.582 1130.696 565.347 1130.696 C 253.111 1130.696 0 877.581 0 565.346 L 1.961 565.346 C 1.961 876.498 254.197 1128.732 565.347 1128.732 Z" fill="rgb(255, 255, 255)" height="1130.6960934794101px" id="if1BmYw1S" transform="translate(92.659 136.321)" width="1130.693351805604px"/></g><g opacity="0.15"><path d="M 466.412 930.861 C 722.923 930.861 930.862 722.922 930.862 466.411 C 930.862 209.905 722.923 1.965 466.412 1.965 C 209.904 1.965 1.961 209.905 1.961 466.411 L 0 466.411 C 0 208.822 208.821 0 466.412 0 C 724.006 0 932.822 208.822 932.822 466.411 C 932.822 724.005 724.006 932.828 466.412 932.828 C 208.821 932.828 0 724.005 0 466.411 L 1.961 466.411 C 1.961 722.922 209.904 930.861 466.412 930.861 Z" fill="rgb(255, 255, 255)" height="932.8284667407987px" id="ef75NsYf6" transform="translate(191.59 235.255)" width="932.8219552655086px"/></g><g opacity="0.5"><path d="M 280.484 0 C 297.399 0 313.63 6.721 325.592 18.685 L 457.817 150.902 C 469.408 162.501 485.135 169.018 501.533 169.017 L 610.964 169.017 C 645.111 169.017 672.799 141.33 672.799 107.182 L 672.799 73.223 L 674.766 73.223 L 674.766 107.182 C 674.766 142.42 646.201 170.978 610.964 170.978 L 501.533 170.978 C 484.614 170.978 468.389 164.257 456.426 152.293 L 324.205 20.076 C 312.611 8.477 296.883 1.961 280.484 1.964 L 0 1.964 L 0 0 Z" fill="url(%23cQ4xRdUtr-2309410982-linear-gradient)" height="170.97763275969464px" id="cQ4xRdUtr" transform="translate(1.173 818.28)" width="674.7656780356198px"/></g><g opacity="0.5"><path d="M 61.263 34.261 L 367.669 34.261 C 384.589 34.261 400.817 40.982 412.783 52.945 L 574.004 214.166 L 572.612 215.554 L 411.395 54.337 C 399.798 42.74 384.069 36.226 367.669 36.228 L 61.263 36.228 C 44.347 36.228 28.116 29.504 16.155 17.54 L 0 1.391 L 1.391 0 L 17.54 16.152 C 29.136 27.747 44.864 34.261 61.263 34.261 Z" fill="url(%23WxV_IOPE7-2309410982-linear-gradient)" height="215.55382175474415px" id="WxV_IOPE7" transform="translate(685.377 854.453)" width="574.0036823012563px"/></g><g opacity="0.5"><path d="M 182.946 552 L 27.577 396.894 C 9.921 379.264 0.002 355.356 0 330.426 L 0 0 L 2.893 0 L 2.893 330.426 C 2.893 354.592 12.509 377.763 29.63 394.851 L 185 549.957 Z" fill="url(%23WwbAIQIz8-2309410982-linear-gradient)" height="552px" id="WwbAIQIz8" transform="translate(484.739 0)" width="185px"/></g><g opacity="0.5"><path d="M 82.446 543.271 C 116.593 543.271 144.281 515.583 144.281 481.435 L 144.281 359.248 C 144.282 342.327 151.004 326.1 162.969 314.135 L 477.103 0 L 478.491 1.387 L 164.356 315.522 C 152.757 327.117 146.241 342.846 146.241 359.248 L 146.241 481.435 C 146.241 516.67 117.683 545.235 82.446 545.235 L 0 545.235 L 0 543.271 Z" fill="url(%23ZWsVQcPfn-2309410982-linear-gradient)" height="545.2346136318063px" id="ZWsVQcPfn" transform="translate(700.405 157.22)" width="478.4906210693257px"/></g><g opacity="0.5"><path d="M 71.95 334.696 L 154.682 334.696 C 197.724 334.696 232.616 369.588 232.616 412.63 L 232.616 495.362 C 232.616 511.764 239.126 527.491 250.725 539.084 L 414.5 702.851 L 413.108 704.243 L 249.338 540.469 C 237.373 528.507 230.651 512.281 230.651 495.362 L 230.651 412.63 C 230.651 370.672 196.64 336.661 154.682 336.661 L 71.95 336.661 C 55.031 336.661 38.805 329.939 26.843 317.974 L 18.683 309.819 C 6.719 297.854 -0.001 281.627 0 264.707 L 0 0 L 1.961 0 L 1.961 264.707 C 1.961 281.105 8.475 296.832 20.07 308.428 L 28.229 316.587 C 39.825 328.182 55.552 334.697 71.95 334.696 Z" fill="url(%23lTyCGrzzP-2309410982-linear-gradient)" height="704.2427839655832px" id="lTyCGrzzP" transform="translate(58.388 199.526)" width="414.49961191971533px"/></g></g></svg>)
A patient calls her clinic at 7:42 on a Tuesday evening to reschedule a post-op visit. She hits a six-option menu, picks "scheduling," waits through a prompt tree, then gets kicked to voicemail. She hangs up. She never rebooks.
That one call, multiplied by the volume of an average practice, is the business case for AI IVR in healthcare. The old touch-tone menu was built for 1995 phone trees. The modern one listens, understands, and books the appointment before the patient finishes her sentence.
This guide walks through what AI IVR actually is, the six use cases with the clearest ROI, the benefits, and how to roll it out without the integration failures that sank the last generation of voice tools. It's written for contact center leaders, patient access directors, practice managers, and CIOs evaluating voice AI now.
What AI IVR in Healthcare Actually Means
AI IVR is an interactive voice response system that uses natural language understanding, speech recognition, and large language models to hold a real conversation with a caller. Instead of "press 1 for scheduling," the caller says what they want and the system handles it.
The three pieces under the hood are automatic speech recognition (ASR), natural language understanding (NLU), and an orchestration layer that connects to the EHR, the scheduling system, and payer portals. The orchestration layer is the hard part. The average hospital runs on 800 different software tools, and the difference between a demo-quality AI IVR and a production-quality one comes down to how many of those systems it can actually read and write to.
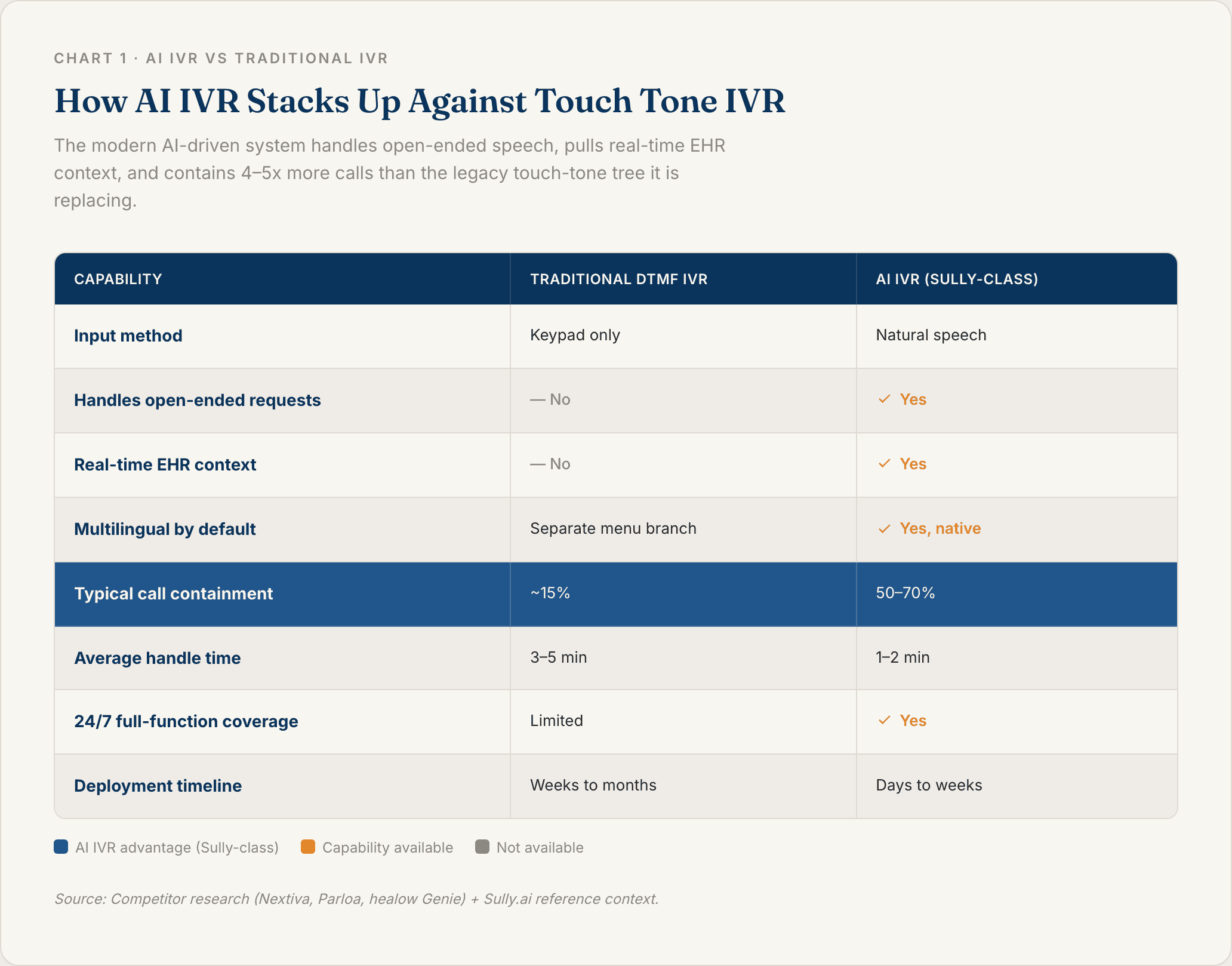
AI IVR vs Traditional Touch Tone IVR
Legacy DTMF IVR (the touch-tone kind) breaks down as soon as a caller has a multi-part question. Ask it to move a Thursday appointment because your daughter is sick, and it hears nothing. Callers abandon multi-level menus at rates of 30 to 50% once the tree goes past three layers.
AI IVR handles open-ended speech, keeps context across turns, and resolves the call end-to-end. The practical difference: traditional IVR contains maybe 15% of calls on its own. Modern AI IVR commonly contains 50 to 70%.
How AI IVR Works on an Inbound Call
Six steps run on every call. The caller connects and gets a greeting. ASR transcribes the speech. NLU identifies intent (refill, reschedule, billing question, triage). The system pulls context from the EHR or scheduling platform. It executes the action (books the slot, queues the refill, routes to a nurse). And it logs the call so the next model version learns.
The line between "AI IVR" and "AI voice agent" is mostly branding. IVR still implies a contact center entry point for inbound calls. Voice agents usually cover both inbound and outbound. Vendors use the terms interchangeably.
Where AI IVR Fits in the Healthcare Contact Center Stack
Think of AI IVR as the phone-channel counterpart to your patient portal chat and SMS reminders. Phones still drive 60 to 70% of patient access volume in most health systems, because portal adoption plateaus, logins break, and older patients prefer to call.
AI IVR is the front door for everyone who will not, or cannot, use the portal. That includes your highest-acuity patients and a meaningful slice of your Medicare population.
Why Healthcare Is Adopting AI IVR Right Now
For every physician seeing patients, there are 10 administrative staff behind them. Most of them are on the phone. Scheduling, refills, referrals, benefits verification. The US healthcare system sits on $250 billion in automatable administrative work every year, and the phone queue is where a huge chunk of that time lives.
Health systems running voice AI have reported reductions of more than 70% in staff time spent on phone-based workflows. That number used to be aspirational. It is now published by operators.
The Cost of a Patient Hitting a Voicemail
No-show rates in primary care run 15 to 30%. A single unrebooked post-op follow-up can cost a practice $200 to $400 in lost revenue, and the readmission risk is worse than the billing hit.
After-hours voicemails convert to rebookings at less than 20%. AI IVR answers on the first ring at 3 a.m., which is why the first-rung ROI calculation almost always pencils out.
Staffing Shortages in Patient Access and Scheduling
Patient access and call-center roles run roughly 20% annual turnover. A new hire takes six to 12 weeks to ramp before they can handle complex calls. AI IVR goes live in days to weeks.
The right framing is not "replace the team." It is "let the team stop answering the same refill question 40 times a day."
Rising Patient Expectations for Self Service
Patients who book rides and return packages on their phone will not tolerate a four-minute hold queue to request a refill. Around two-thirds of patients now prefer self-service for routine tasks, but they still pick up the phone when the portal login breaks or the question feels urgent.
AI IVR is what you put on the other end of that call.
Top AI IVR Use Cases in Healthcare
The six use cases below are the ones with the clearest published ROI. Sequence matters. Start with the high-volume, low-complexity ones. Work toward the clinical-adjacent ones only once the easier workflows are stable.
Appointment Scheduling and Rescheduling
The most common deployment. AI IVR reads calendar availability from the EHR or scheduling system in real time, confirms insurance coverage for the visit type, and books the slot on the same call.
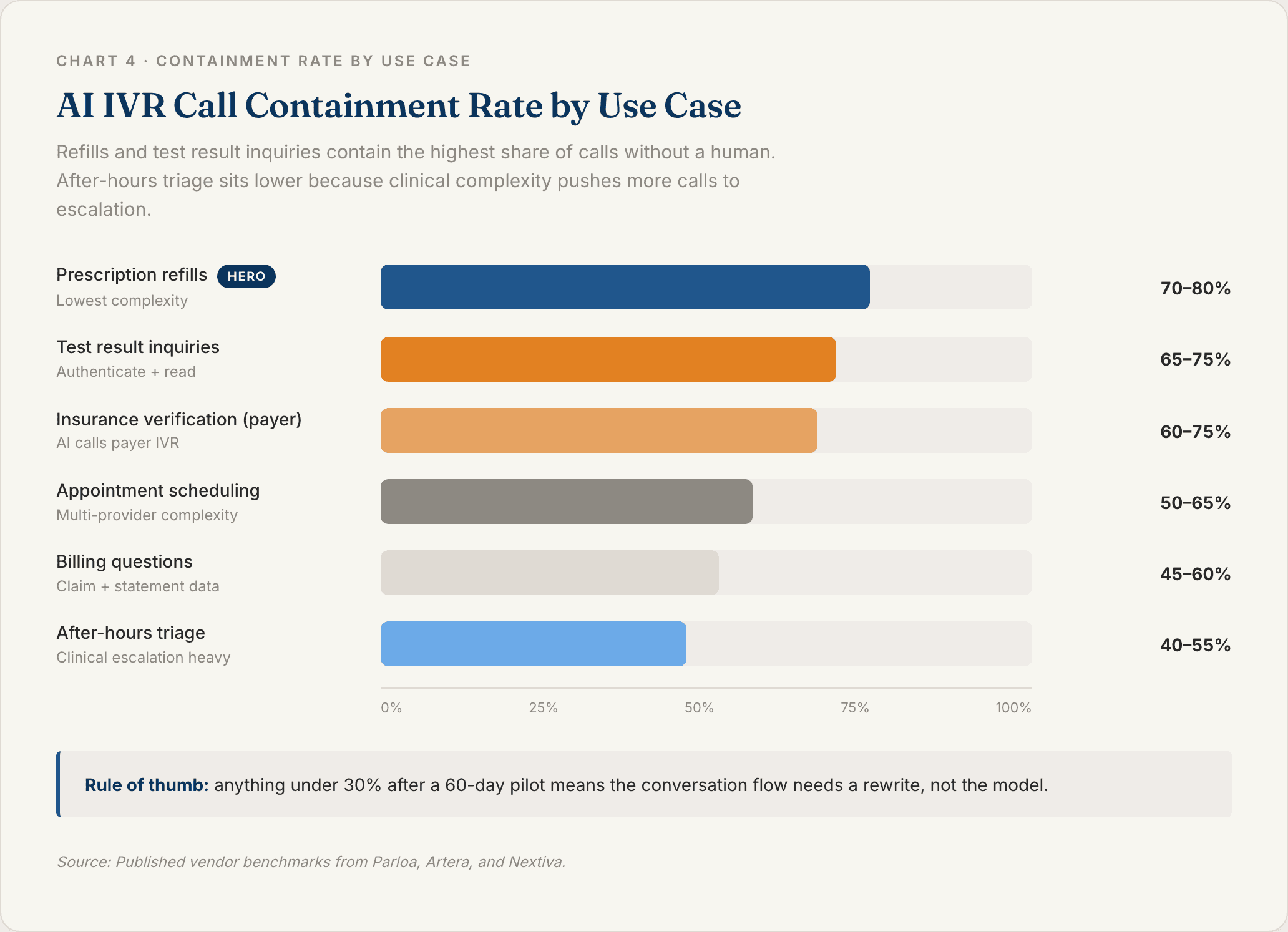
Multi-provider, multi-location practices see the biggest lift, because the traditional phone tree collapses once you ask a caller to pick a provider, pick a location, and pick a visit type. Containment rates on scheduling intents land between 50 and 65% in most deployments.
Prescription Refill Requests
Refills are the highest-volume, lowest-complexity call in most primary care practices. The AI captures the drug name, confirms the pharmacy, checks the EHR for last-fill date, routes to the right provider for approval, and texts the patient when it is ready.
This is usually the first use case a practice automates. Containment rates run 70 to 80%.
Insurance and Benefits Verification
For payer-facing calls (eligibility, prior auth status, claim status), AI IVR flips the usual pattern. The AI is the caller, not the answerer. It navigates the payer's own IVR, waits on hold, and returns structured data to the billing team.
Prosper AI is one published example. This use case is underrated. It does not touch a patient, so the compliance lift is different, and the hours recovered land directly in revenue cycle.
After Hours Triage and Nurse Line Routing
Outside business hours, AI IVR collects symptom information, applies a triage protocol, and either books a same-day appointment, routes to the on-call nurse, or directs to the ED for emergencies.
This is the use case most tied to patient safety. AI IVR should not diagnose. It should sort. And every triage deployment needs a one-phrase escape route to a human.
Test Results and Billing Inquiries
Low-acuity, high-volume. Patients call about lab results they already have in the portal (they missed the notification) and billing questions that are usually answerable from claim data. The AI authenticates the caller, reads the result summary or statement, and escalates only when the question is actually complex.
Containment rates on these intents typically exceed 65%.
Post Discharge Follow Up and Care Gap Outreach
The outbound use case. AI IVR calls discharged patients to confirm medication pickup, check on symptoms, and book the seven-day follow-up. For value-based care contracts, the same system runs annual wellness visit outreach and preventive screening reminders.
Published deployments from Artera and others report the 70%+ staff-time reduction in this category. Outbound is where the ROI math gets most dramatic, because human agents cannot cost-effectively call 5,000 post-discharge patients a month.
Benefits of AI IVR for Healthcare Organizations
Three buckets: cost, capacity, and patient experience. The cost story is the loudest. The capacity story is more important.
24/7 Patient Access Without 24/7 Staffing
AI IVR answers every call instantly. Time of day does not matter. Call volume spikes do not matter. Monday-morning surges stop requiring Monday-morning overstaffing, and 3 a.m. coverage stops requiring an on-call nurse to pick up refill questions.
This is capacity expansion, not headcount reduction. The patients who used to hang up now get rebooked.
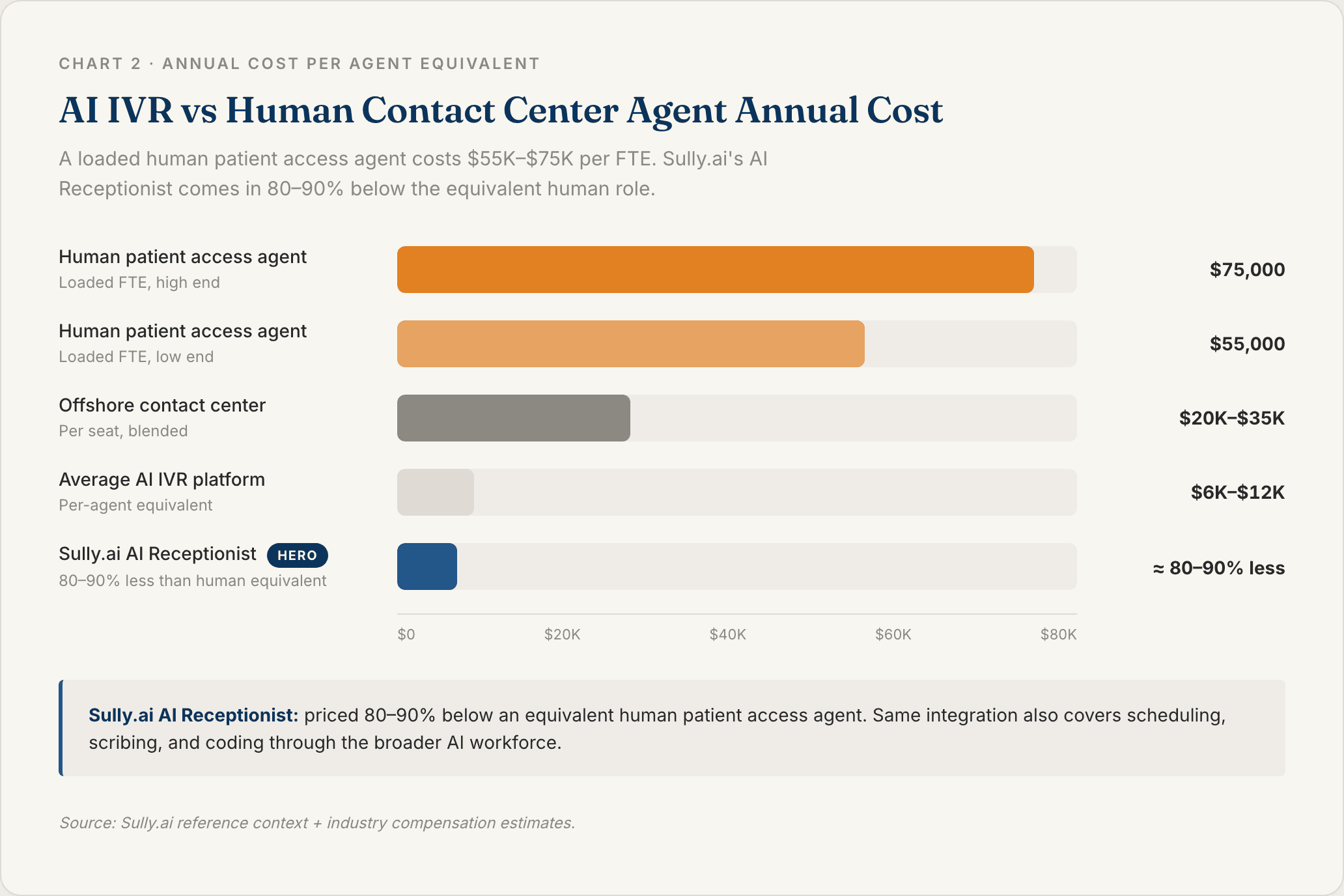
Cost Reduction Compared to Human Contact Center Agents
Each Sully AI role costs 80 to 90% less than the equivalent human role. For a 20-agent contact center, that is a multi-million-dollar annual swing. Realistic deployments keep humans for complex cases and route the repetitive 60 to 70% of volume to AI.
Shorter Hold Times and Higher First Call Resolution
McKinsey estimates AI-driven contact center automation can handle up to 30% more calls with fewer agents. First call resolution also improves, because the AI has real-time EHR and scheduling context that human agents usually have to look up manually mid-call.
The patient gets a faster answer. The practice gets a cleaner metric.
HIPAA Compliant Patient Interactions at Scale
Every interaction is logged, transcribed, and auditable. Reputable vendors sign a BAA, encrypt data in transit and at rest, and restrict how call data is used for model training.
HIPAA compliance is a pass/fail gate, not a feature bullet. If the vendor cannot answer BAA and encryption questions cleanly in the first meeting, move on.
Multilingual Support Without Bilingual Hiring
AI IVR handles Spanish, Mandarin, Vietnamese, and other languages on the same phone number. No "press 2 for Spanish" detour. No interpreter-line cost for routine calls. For health systems serving multilingual patient populations, this is often the fastest-to-measure improvement in patient satisfaction.
How to Implement AI IVR in Healthcare
Most failed deployments fail on integration depth, not AI quality. The model is not usually the bottleneck. The EHR connection is.
1. Map Your Highest Volume Call Intents
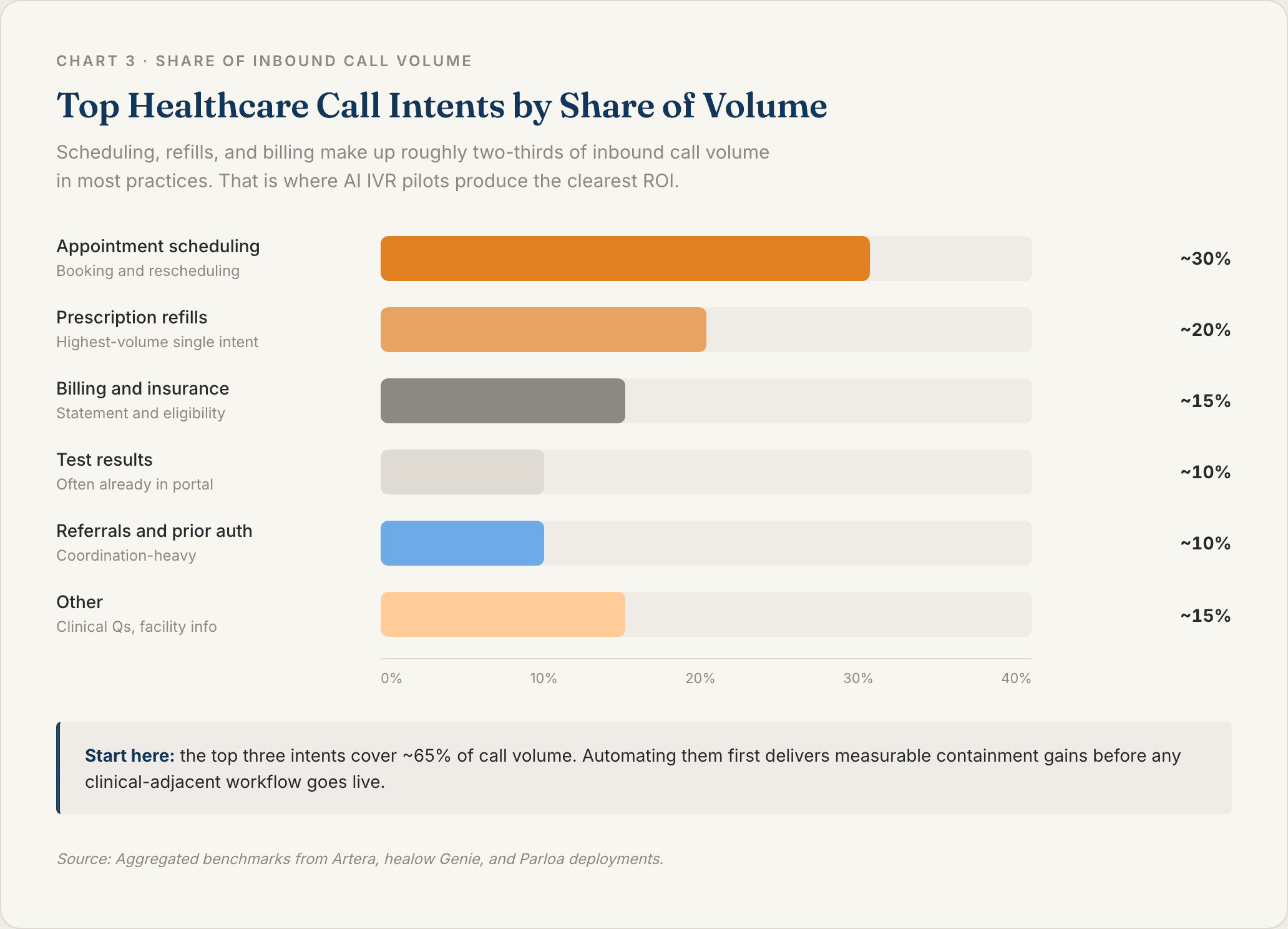
Pull 30 days of call logs or ask your patient access supervisor for the top 10 reasons patients call. In most practices, scheduling, refills, and billing make up 60 to 70% of volume.
Start there. Do not start with the edge cases.
2. Pick a HIPAA Compliant Platform With EHR Integration
Evaluate vendors on BAA coverage, integration depth with your specific EHR (Epic, Cerner, Meditech, Athenahealth), and whether they support your scheduling system's real-time availability API.
Surface-level API access is not the same as production-grade integration. Ask to see a live read/write to a sandbox EHR in the demo. If the vendor refuses, that tells you everything.
3. Design Conversation Flows, Not Menu Trees
The biggest design mistake is porting the old DTMF tree into an AI wrapper. "Say scheduling, say refill, say billing" is just touch-tone with a microphone.
Let callers state intent in open-ended language. Keep conversations to three to five turns before the AI either completes the task or escalates. Every extra turn is a place patients drop out.
4. Build a Clear Human Escalation Path
Every deployment needs a one-phrase escape ("talk to a person") that routes to a live agent during business hours and to a callback queue after hours.
Patient trust depends on the exit door being obvious. Hiding the human option to juice containment numbers is a short-term win that ends in bad surveys.
5. Pilot on a Single Intent Before Rolling Out Broadly
Start with refills or scheduling on one clinic or call queue. Measure containment, CSAT, and appointment conversion for 30 to 60 days. Expand to the next intent only after the first one clears its KPIs.
Phased rollouts beat big-bang cutovers in every published deployment.
6. Measure Containment Rate, Appointment Conversion, and Patient CSAT
Three metrics matter. Containment rate is the percentage of calls resolved without a human. Appointment conversion is the percentage of scheduling intents that actually result in a booked visit. Patient CSAT is collected via a post-call SMS survey.
Industry-benchmark containment sits between 40 and 70%, depending on the intent. Anything below 30% after pilot means the conversation flow needs a rewrite.
Build Your AI Workforce With Sully.ai
Most AI IVR vendors sold tools. Each one solves one problem. None of them talk to each other. Sully.ai built a workforce instead.
The AI Receptionist handles inbound scheduling, refills, and after-hours triage. The AI Scribe captures the visit. The AI Coder turns the note into a clean claim. The AI Triage Nurse runs pre-visit intake and post-visit follow-up. They share context and hand off cases automatically. When the Receptionist books a post-op follow-up, the Scribe already has the context from the last visit and the Coder has already submitted the claim.
Sully runs on a single EHR integration. Integrate once, and it works with Epic, Cerner, Meditech, and Athenahealth. That is the part that most voice AI projects never get to.
The numbers: 5,000+ providers across multiple specialties, 50M+ hours of AI work delivered, each AI role priced 80 to 90% less than the human equivalent.
If your patient access team is drowning and your phone tree is losing you appointments every night, book a demo. Come with your top three call intents. You will see all of them answered live in the meeting.
FAQ
What is AI IVR in healthcare?
AI IVR in healthcare is a phone system that uses natural language understanding and real-time EHR integration to handle patient calls conversationally. It schedules appointments, processes refill requests, verifies insurance, and triages after-hours concerns without forcing callers through a touch-tone menu tree. Platforms like Sully.ai's AI Receptionist go further by sharing context with an AI Scribe, Coder, and Triage Nurse, so the whole patient interaction is handled as a coordinated workflow rather than an isolated call.
How is AI IVR different from traditional IVR?
Traditional IVR uses keypad menus and breaks down as soon as callers have complex or multi-part requests. AI IVR uses speech recognition and large language models to handle open-ended conversation, ask clarifying questions, and complete workflows end-to-end. The practical difference: traditional IVR contains around 15% of calls. Modern AI IVR commonly contains 50 to 70%.
Is AI IVR HIPAA compliant?
AI IVR can be HIPAA compliant, but it is not compliant by default. The vendor has to sign a Business Associate Agreement (BAA), encrypt data in transit and at rest, log all interactions for audit, and restrict how call data is used for model training. Treat HIPAA compliance as a pass/fail gate during vendor evaluation, not a feature to negotiate later.
How much does AI IVR cost compared to a human call center?
Each AI agent role typically runs 80 to 90% less than the equivalent human role once fully deployed, though realistic deployments run AI alongside human staff rather than replacing them entirely. For a mid-sized practice with a 5-person patient access team handling roughly 20,000 calls a month, AI IVR can shift the cost structure meaningfully inside the first year.
What use cases should a healthcare organization automate first with AI IVR?
Start with the highest-volume, lowest-complexity intents: prescription refill requests, appointment scheduling, and simple billing or test result inquiries. Those usually make up 60 to 70% of call volume and carry minimal clinical risk. Once they clear their containment and CSAT targets, expand to after-hours triage, post-discharge follow-up, and care gap outreach.
TABLE OF CONTENTS
Hire your
Medical AI Team
Take a look at our Medical AI Team
AI Receptionist
Manages patient scheduling, communications, and front-desk operations across all channels.
AI Scribe
Documents clinical encounters and maintains accurate EHR/EMR records in real-time.
AI Medical Coder
Assigns and validates medical codes to ensure accurate billing and regulatory compliance.
AI Nurse
Assesses patient urgency and coordinates appropriate care pathways based on clinical needs.