"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="WxV_IOPE7-2309410982-linear-gradient" x1="1" x2="0" y1="0.5951279047551217" y2="0.4048720952448783"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="WwbAIQIz8-2309410982-linear-gradient" x1="0.43478742751482424" x2="0.6358595260107829" y1="0.26" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="ZWsVQcPfn-2309410982-linear-gradient" x1="0.9508213454678907" x2="0.04917865453210929" y1="0" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="lTyCGrzzP-2309410982-linear-gradient" x1="0.374937164194436" x2="0.625062835805564" y1="0" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient></defs><g d="M 658.002 1357.705 C 1020.321 1357.705 1314.04 1063.989 1314.04 701.667 C 1314.04 339.347 1020.321 45.626 658.002 45.626 C 295.681 45.626 1.96 339.347 1.96 701.667 L 0 701.667 C 0 338.263 294.598 43.665 658.002 43.665 C 1021.404 43.665 1316 338.263 1316 701.667 C 1316 1065.072 1021.404 1359.672 658.002 1359.672 C 294.598 1359.672 0 1065.072 0 701.667 L 1.96 701.667 C 1.96 1063.989 295.681 1357.705 658.002 1357.705 Z M 658.005 1265.053 C 969.154 1265.053 1221.392 1012.819 1221.392 701.667 C 1221.392 390.517 969.154 138.281 658.005 138.281 C 346.856 138.281 94.619 390.517 94.619 701.667 L 92.659 701.667 C 92.659 389.433 345.77 136.321 658.005 136.321 C 970.241 136.321 1223.352 389.433 1223.352 701.667 C 1223.352 1013.902 970.241 1267.017 658.005 1267.017 C 345.77 1267.017 92.659 1013.902 92.659 701.667 L 94.619 701.667 C 94.619 1012.819 346.856 1265.053 658.005 1265.053 Z M 658.002 1166.116 C 914.513 1166.116 1122.452 958.178 1122.452 701.667 C 1122.452 445.16 914.513 237.22 658.002 237.22 C 401.494 237.22 193.551 445.16 193.551 701.667 L 191.59 701.667 C 191.59 444.077 400.411 235.255 658.002 235.255 C 915.596 235.255 1124.412 444.077 1124.412 701.667 C 1124.412 959.261 915.596 1168.084 658.002 1168.084 C 400.411 1168.084 191.59 959.261 191.59 701.667 L 193.551 701.667 C 193.551 958.178 401.494 1166.116 658.002 1166.116 Z M 281.657 818.28 C 298.572 818.28 314.804 825.001 326.765 836.965 L 458.99 969.182 C 470.582 980.781 486.308 987.298 502.706 987.298 L 612.137 987.298 C 646.284 987.298 673.972 959.61 673.972 925.463 L 673.972 891.504 L 675.939 891.504 L 675.939 925.463 C 675.939 960.7 647.374 989.258 612.137 989.258 L 502.706 989.258 C 485.788 989.258 469.562 982.537 457.599 970.573 L 325.378 838.356 C 313.785 826.757 298.056 820.242 281.657 820.244 L 1.173 820.244 L 1.173 818.28 Z M 746.64 888.714 L 1053.046 888.714 C 1069.967 888.714 1086.194 895.435 1098.16 907.398 L 1259.381 1068.619 L 1257.99 1070.007 L 1096.772 908.79 C 1085.175 897.193 1069.446 890.679 1053.046 890.681 L 746.64 890.681 C 729.724 890.681 713.493 883.957 701.533 871.993 L 685.377 855.845 L 686.769 854.453 L 702.917 870.605 C 714.513 882.201 730.241 888.715 746.64 888.714 Z M 667.685 552 L 512.316 396.894 C 494.66 379.264 484.741 355.356 484.739 330.426 L 484.739 0 L 487.632 0 L 487.632 330.426 C 487.632 354.592 497.248 377.763 514.369 394.851 L 669.739 549.957 Z M 782.851 700.491 C 816.998 700.491 844.686 672.804 844.686 638.655 L 844.686 516.468 C 844.687 499.547 851.409 483.32 863.374 471.355 L 1177.508 157.22 L 1178.896 158.607 L 864.762 472.742 C 853.162 484.337 846.646 500.067 846.646 516.468 L 846.646 638.655 C 846.646 673.89 818.088 702.455 782.851 702.455 L 700.405 702.455 L 700.405 700.491 Z M 130.338 534.223 L 213.07 534.223 C 256.112 534.223 291.003 569.114 291.003 612.156 L 291.003 694.888 C 291.003 711.29 297.514 727.017 309.113 738.611 L 472.887 902.378 L 471.496 903.769 L 307.726 739.995 C 295.761 728.033 289.038 711.807 289.038 694.888 L 289.038 612.156 C 289.038 570.198 255.028 536.188 213.07 536.188 L 130.338 536.188 C 113.419 536.187 97.193 529.465 85.23 517.5 L 77.071 509.345 C 65.107 497.381 58.386 481.153 58.388 464.233 L 58.388 199.526 L 60.348 199.526 L 60.348 464.233 C 60.349 480.631 66.863 496.358 78.458 507.954 L 86.617 516.113 C 98.213 527.709 113.94 534.223 130.338 534.223 Z" fill="transparent" height="1359.6717183844698px" id="DcyumyANr" transform="translate(0 -43.665)" width="1316px"><g opacity="0.5"><path d="M 658.002 1314.039 C 1020.321 1314.039 1314.04 1020.324 1314.04 658.001 C 1314.04 295.681 1020.321 1.961 658.002 1.961 C 295.681 1.961 1.96 295.682 1.96 658.001 L 0 658.001 C 0 294.598 294.598 0 658.002 0 C 1021.404 0 1316 294.598 1316 658.001 C 1316 1021.407 1021.404 1316.007 658.002 1316.007 C 294.598 1316.007 0 1021.407 0 658.001 L 1.96 658.001 C 1.96 1020.324 295.681 1314.039 658.002 1314.039 Z" fill="rgb(255, 255, 255)" height="1316.0065114752902px" id="dxf13D52Y" transform="translate(0 43.665)" width="1316px"/></g><g opacity="0.3"><path d="M 565.347 1128.732 C 876.496 1128.732 1128.733 876.498 1128.733 565.346 C 1128.733 254.196 876.496 1.961 565.347 1.961 C 254.197 1.961 1.961 254.196 1.961 565.346 L 0 565.346 C 0 253.112 253.111 0 565.347 0 C 877.582 0 1130.693 253.112 1130.693 565.346 C 1130.693 877.581 877.582 1130.696 565.347 1130.696 C 253.111 1130.696 0 877.581 0 565.346 L 1.961 565.346 C 1.961 876.498 254.197 1128.732 565.347 1128.732 Z" fill="rgb(255, 255, 255)" height="1130.6960934794101px" id="if1BmYw1S" transform="translate(92.659 136.321)" width="1130.693351805604px"/></g><g opacity="0.15"><path d="M 466.412 930.861 C 722.923 930.861 930.862 722.922 930.862 466.411 C 930.862 209.905 722.923 1.965 466.412 1.965 C 209.904 1.965 1.961 209.905 1.961 466.411 L 0 466.411 C 0 208.822 208.821 0 466.412 0 C 724.006 0 932.822 208.822 932.822 466.411 C 932.822 724.005 724.006 932.828 466.412 932.828 C 208.821 932.828 0 724.005 0 466.411 L 1.961 466.411 C 1.961 722.922 209.904 930.861 466.412 930.861 Z" fill="rgb(255, 255, 255)" height="932.8284667407987px" id="ef75NsYf6" transform="translate(191.59 235.255)" width="932.8219552655086px"/></g><g opacity="0.5"><path d="M 280.484 0 C 297.399 0 313.63 6.721 325.592 18.685 L 457.817 150.902 C 469.408 162.501 485.135 169.018 501.533 169.017 L 610.964 169.017 C 645.111 169.017 672.799 141.33 672.799 107.182 L 672.799 73.223 L 674.766 73.223 L 674.766 107.182 C 674.766 142.42 646.201 170.978 610.964 170.978 L 501.533 170.978 C 484.614 170.978 468.389 164.257 456.426 152.293 L 324.205 20.076 C 312.611 8.477 296.883 1.961 280.484 1.964 L 0 1.964 L 0 0 Z" fill="url(%23cQ4xRdUtr-2309410982-linear-gradient)" height="170.97763275969464px" id="cQ4xRdUtr" transform="translate(1.173 818.28)" width="674.7656780356198px"/></g><g opacity="0.5"><path d="M 61.263 34.261 L 367.669 34.261 C 384.589 34.261 400.817 40.982 412.783 52.945 L 574.004 214.166 L 572.612 215.554 L 411.395 54.337 C 399.798 42.74 384.069 36.226 367.669 36.228 L 61.263 36.228 C 44.347 36.228 28.116 29.504 16.155 17.54 L 0 1.391 L 1.391 0 L 17.54 16.152 C 29.136 27.747 44.864 34.261 61.263 34.261 Z" fill="url(%23WxV_IOPE7-2309410982-linear-gradient)" height="215.55382175474415px" id="WxV_IOPE7" transform="translate(685.377 854.453)" width="574.0036823012563px"/></g><g opacity="0.5"><path d="M 182.946 552 L 27.577 396.894 C 9.921 379.264 0.002 355.356 0 330.426 L 0 0 L 2.893 0 L 2.893 330.426 C 2.893 354.592 12.509 377.763 29.63 394.851 L 185 549.957 Z" fill="url(%23WwbAIQIz8-2309410982-linear-gradient)" height="552px" id="WwbAIQIz8" transform="translate(484.739 0)" width="185px"/></g><g opacity="0.5"><path d="M 82.446 543.271 C 116.593 543.271 144.281 515.583 144.281 481.435 L 144.281 359.248 C 144.282 342.327 151.004 326.1 162.969 314.135 L 477.103 0 L 478.491 1.387 L 164.356 315.522 C 152.757 327.117 146.241 342.846 146.241 359.248 L 146.241 481.435 C 146.241 516.67 117.683 545.235 82.446 545.235 L 0 545.235 L 0 543.271 Z" fill="url(%23ZWsVQcPfn-2309410982-linear-gradient)" height="545.2346136318063px" id="ZWsVQcPfn" transform="translate(700.405 157.22)" width="478.4906210693257px"/></g><g opacity="0.5"><path d="M 71.95 334.696 L 154.682 334.696 C 197.724 334.696 232.616 369.588 232.616 412.63 L 232.616 495.362 C 232.616 511.764 239.126 527.491 250.725 539.084 L 414.5 702.851 L 413.108 704.243 L 249.338 540.469 C 237.373 528.507 230.651 512.281 230.651 495.362 L 230.651 412.63 C 230.651 370.672 196.64 336.661 154.682 336.661 L 71.95 336.661 C 55.031 336.661 38.805 329.939 26.843 317.974 L 18.683 309.819 C 6.719 297.854 -0.001 281.627 0 264.707 L 0 0 L 1.961 0 L 1.961 264.707 C 1.961 281.105 8.475 296.832 20.07 308.428 L 28.229 316.587 C 39.825 328.182 55.552 334.697 71.95 334.696 Z" fill="url(%23lTyCGrzzP-2309410982-linear-gradient)" height="704.2427839655832px" id="lTyCGrzzP" transform="translate(58.388 199.526)" width="414.49961191971533px"/></g></g></svg>)
Every nurse runs a head to toe assessment on every patient, every shift. Miss a step, and you can miss a stroke, a clot, or a pressure injury forming under the sheets.
This guide is the single reference you can scroll through at the bedside. You get the definition, prep, techniques, the full checklist by body system, documentation rules, and how AI now takes the charting off your plate.
What a Head-to-Toe Assessment Is in Nursing Practice
A head to toe assessment is a systematic, top-down physical exam that checks every major body system in the same order, every time. Nurses use it to set a baseline at admission, to catch changes at the start of a shift, and to confirm a patient is stable after a procedure.
A typical shift assessment on a stable patient takes 10 to 15 minutes. A full admission assessment can run 25 to 30 minutes because it includes a complete history and medication review.
Not every assessment has the same purpose. There are three common types, and knowing which one you are doing shapes how deep you go.
Complete Health Assessment
This is the full baseline. You do it on admission, at annual physicals, or any time a patient enters a new care setting. Every system gets examined in sequence, and you spend real time on history.
Problem-Focused Assessment
This one is narrow. The chief complaint drives where you look. Chest pain sends you straight to the cardiopulmonary exam. New weakness sends you to a neuro focus. You still scan the rest, but you zoom in on the system in question.
Ongoing Shift Assessment
Most bedside RNs mean this one when they say “head to toe.” It is the abbreviated version you run at the start of every 12-hour shift. The goal is to set your own baseline so any change later in the shift stands out.
Equipment and Patient Preparation Before Starting
Good preparation is where new nurses lose the most time. You assemble tools, set up the room, and get the patient on board before you ever place a stethoscope.
Required Equipment Checklist
Keep this kit ready at the bedside:
Stethoscope
Penlight
Thermometer
Blood pressure cuff
Pulse oximeter
Watch with a second hand
Gloves and hand sanitizer
Reflex hammer
Tuning fork
Tongue depressor
Tape measure
Snellen chart
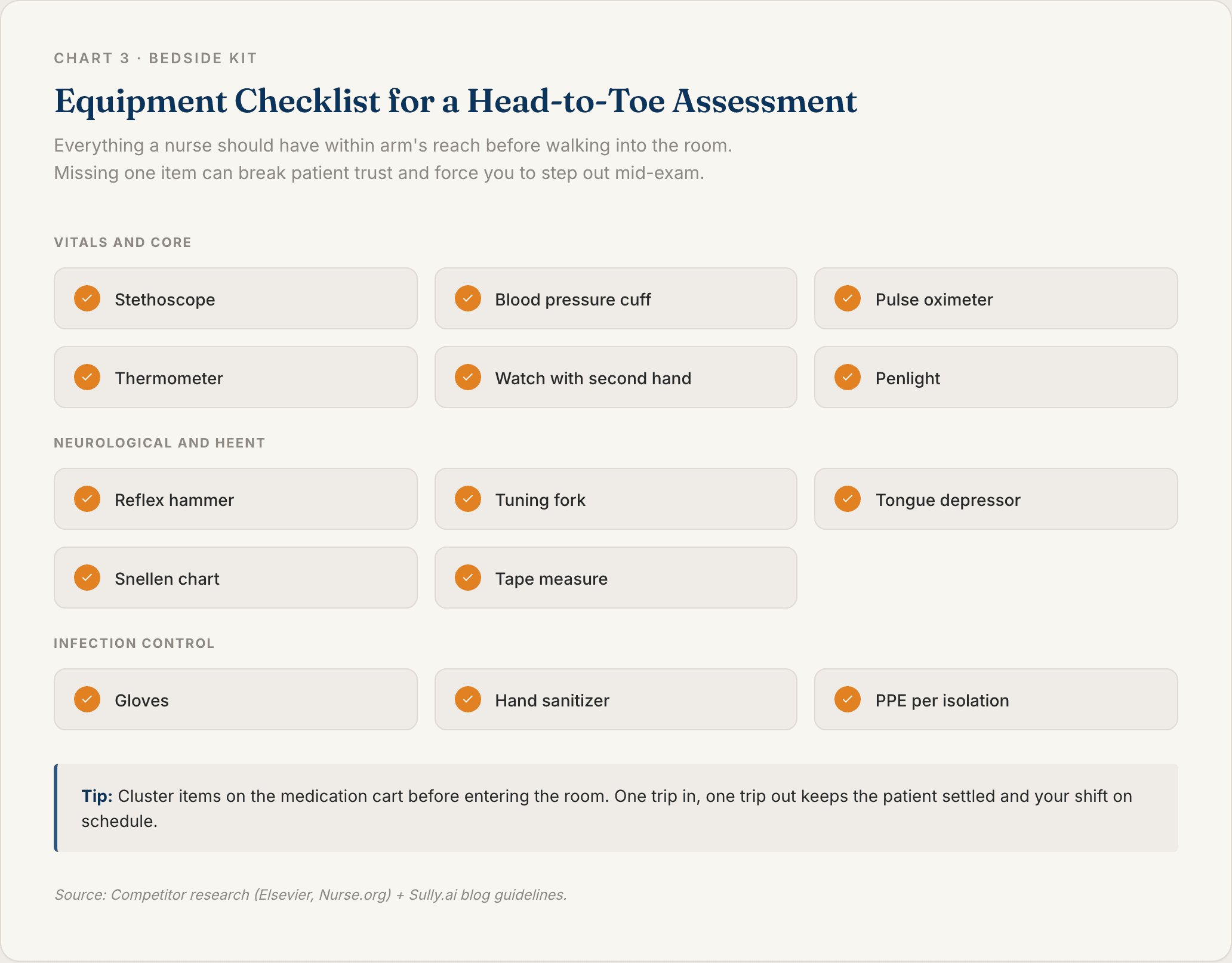
Most hospitals stock these on the medication cart or at the bedside. If your unit is missing anything, grab it before you walk in. Stepping out mid-exam breaks patient trust and wastes time.
Setting Up the Environment
Close the curtain. Get the room warm, since your patient will be partially exposed. Raise the bed to your waist height to protect your back. Good lighting is not optional for skin and eye checks.
Patient Identification and Consent
Verify two identifiers: name and date of birth. Then explain what you are about to do in plain language, and ask for verbal consent. For sensitive exams, offer a chaperone.
Infection Control Steps
Wash your hands before and after contact, every time. Wear PPE that matches the patient’s isolation status. Wipe your stethoscope diaphragm between patients, since it lives on your neck all day and picks up everything.
Four Core Techniques for Physical Examination
Nurses use four techniques on every exam: inspection, palpation, percussion, and auscultation (IPPA). You apply them in that order on every body system, with one famous exception you will meet below.
Inspection
Look first, always. You check color, symmetry, lesions, swelling, and signs of distress. A trained eye catches most problems before a hand ever touches the patient.
Palpation
Touch with purpose. Use your fingertips for fine detail, your palms for broad areas like the abdomen, and the back of your hand for temperature. Light palpation goes about 1 cm deep. Deep palpation goes about 4 cm, and only after light is clear.
Percussion
Tap to read what is underneath. Dull sounds sit over solid organs. Resonant sounds come from air-filled lungs. Tympanic sounds come from air in the bowel. Routine shift assessments skip percussion often, but it is a core skill for focused exams.
Auscultation
Listen with the right side of the stethoscope. The diaphragm catches high-pitched sounds like lung and bowel sounds. The bell catches low-pitched sounds like heart murmurs and bruits. Warm the metal before it touches skin. Your patient will thank you.
The one exception: on the abdomen, the order flips to inspect, auscultate, percuss, palpate. Pressing on the belly first alters bowel sounds, so you listen before you touch. This comes up on the NCLEX. Do not forget it.
Head-to-Toe Assessment Checklist by Body System
This is the core of the exam. You move top down, left to right, comparing one side to the other as you go. Run the same sequence on every patient and your brain starts catching changes you would otherwise miss.
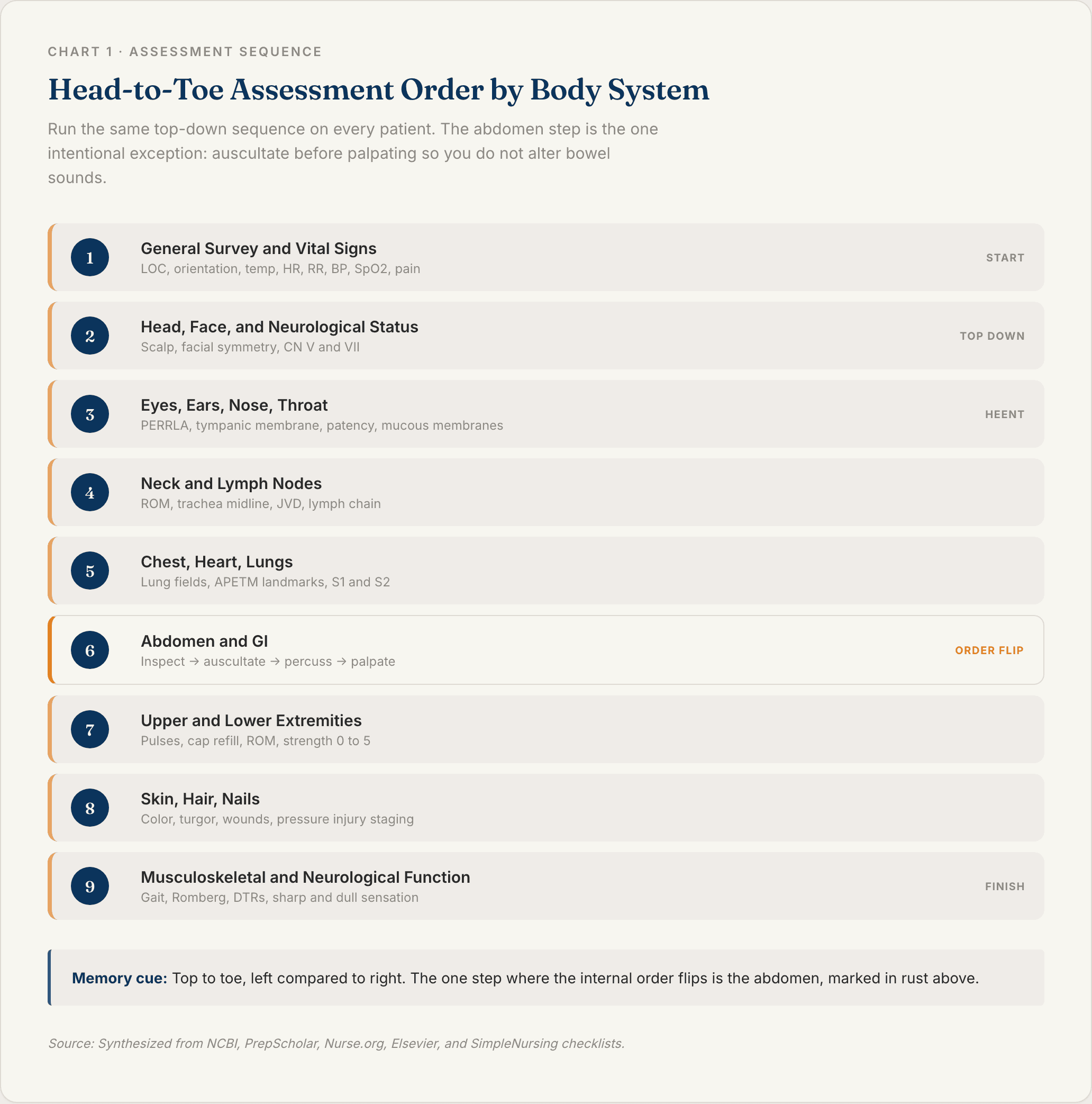
General Survey and Vital Signs
Start here before you touch the patient. You are reading the room.
Level of consciousness using AVPU or Glasgow Coma Scale
Orientation x 4 to person, place, time, and situation
General appearance, posture, gait, hygiene, affect
Vitals: temperature, heart rate, respiratory rate, blood pressure, SpO2
Pain on a 0 to 10 scale
Head, Face, and Neurological Status
Move to the scalp and face. Inspect hair distribution. Palpate the skull for tenderness and lesions. Check facial symmetry (cranial nerve VII) by asking the patient to smile and raise eyebrows. Test sharp and dull sensation on the face (cranial nerve V).
Eyes, Ears, Nose, and Throat
This is the HEENT block, and it is where new nurses tend to rush. Slow down.
Eyes: PERRLA (pupils equal, round, reactive to light and accommodation), six cardinal gazes, Snellen chart if vision is a concern
Ears: inspect the auricle, check the tympanic membrane, run a whisper test for basic hearing
Nose: confirm patency of both nostrils, check the septum is midline
Mouth and throat: moist mucous membranes, tongue midline, uvula midline, tonsils graded
Neck and Lymph Nodes
Check range of motion in all directions. Palpate the trachea, which should sit midline. Assess for jugular vein distension with the head of bed at 45 degrees. Palpate lymph nodes in order: preauricular, postauricular, occipital, submandibular, cervical chain, supraclavicular, axillary. Shoulder shrug against resistance tests cranial nerve XI.
Chest, Heart, and Lungs
Inspect the chest wall for symmetry and respiratory effort. Auscultate lung fields front and back at the apices, mid-chest, and bases. Listen to the heart at the five classic landmarks using the APETM memory hook: aortic, pulmonic, Erb’s point, tricuspid, and mitral. Note S1 and S2. Flag any murmurs, rubs, or extra sounds.
Abdomen and Gastrointestinal System
Remember the order flip here: inspect, auscultate, percuss, palpate. Listen to all four quadrants for bowel sounds before you press anywhere. Then do light palpation, and only go to deep palpation if light is painless. Ask about last bowel movement, appetite, and any nausea.
Upper and Lower Extremities
Inspect for edema, cyanosis, and lesions. Palpate pulses bilaterally: radial, brachial, femoral, popliteal, dorsalis pedis, posterior tibial. Grade each pulse 0 to 4+. Capillary refill should be under three seconds. Check range of motion and muscle strength on a 0 to 5 scale on both sides.
Skin, Hair, and Nails
Assess color, turgor, temperature, and moisture across every area you expose. Note any rashes, wounds, or pressure injuries, and stage any pressure injuries you find. Check the nail beds for color, clubbing, and capillary refill. If the patient is at risk, run a Braden score.
Musculoskeletal and Neurological Function
Observe gait and balance if the patient is ambulatory. Run a Romberg test if indicated. Check deep tendon reflexes at the biceps, triceps, patellar, and Achilles sites, and grade them 0 to 4+. Test sharp versus dull sensation and light touch on the extremities.
Documentation Standards for Nursing Assessments
An assessment you do not chart is an assessment that did not happen. Documentation turns your exam into the legal record the next nurse, the provider, and the billing team all rely on.
Objective vs Subjective Findings
Objective is what you observed, measured, or heard. Subjective is what the patient told you, and you write it in their own words using quotes. Never mix the two in the same sentence.
Example: “Patient reports ‘8 out of 10’ sharp pain in right lower quadrant. Abdomen firm to deep palpation, bowel sounds hypoactive in all four quadrants.”
SOAP Note Format
Most EHRs chart in SOAP: Subjective, Objective, Assessment, Plan. Your head to toe findings live in the Objective line. Patient-reported symptoms live in Subjective. Your clinical impression goes in Assessment. Next steps go in Plan.
Charting Abnormal Findings
Describe what you see, not what you think caused it. Write “3 cm erythematous, non-blanching area on sacrum,” not “looks like a pressure ulcer.” The provider is the one who makes the diagnosis. You notify them when a finding is outside the patient’s baseline.
Common Mistakes and Tips for a Thorough Assessment
A preceptor will tell you the checklist is only half the job. The other half is the small habits that catch problems early.
Maintaining Bilateral Symmetry Checks
Compare left to right on everything: pulses, reflexes, strength, skin color, pupil response. Asymmetry is often the first sign of a neuro or vascular issue. Assess both sides in the same breath, not with a five-minute gap in between.
Communicating Throughout the Exam
Narrate each step out loud. “I’m going to listen to your lungs now. Can you take a deep breath for me?” It calms the patient, signals professionalism, and gives you a live read on their cognitive status.
Time Management in a Busy Shift
Target 10 to 15 minutes for a routine shift assessment on a stable patient. Cluster your care: medications, assessment, and morning hygiene in a single room visit. Fewer room entries means less disruption for the patient and more time for your next task.
Modernizing Head-to-Toe Assessments with AI Support
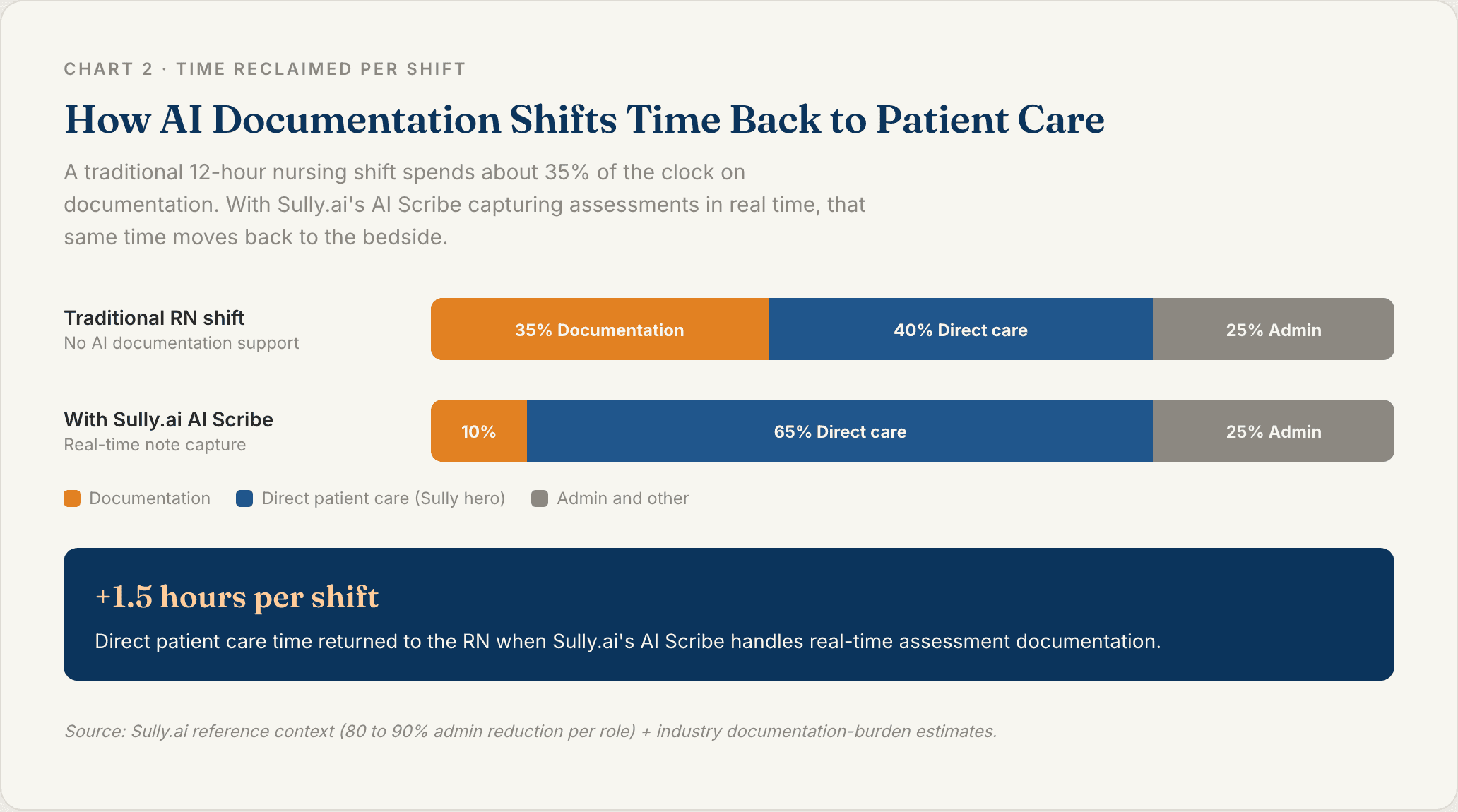
Here is the part most assessment guides skip. Nurses spend a huge portion of every shift on documentation instead of patient care. The US has an estimated $250 billion in automatable administrative work in healthcare every year, and a big chunk of it is charting that nurses do after the patient interaction is already over.
AI employees are starting to shoulder that load. They do not replace the nurse at the bedside. They take charting, intake, and scheduling off the nurse so the head to toe itself gets the full attention it deserves.
AI Scribes for Real-Time Assessment Documentation
Sully.ai’s AI Scribe captures the assessment as you narrate it. You finish the exam, the note is already in the EHR. No end-of-shift charting backlog. Sully plugs in through a single EHR integration that works with Epic, Cerner, Meditech, and Athenahealth, so you are not rebuilding the connection for every specialty.
AI Triage Nurse for Pre-Visit Intake
Sully’s AI Triage Nurse collects symptoms, history, and medication reconciliation before you walk into the room. Your chart is pre-populated. The head to toe starts with context, not data entry, and you catch things in the first minute that used to take 10.
How Sully.ai Supports Bedside Nurses
Sully is not one tool. It is a coordinated workforce of AI employees that share context and hand off cases: Scribe, Triage Nurse, Receptionist, and Coder. For every physician seeing patients, there are 10 administrative staff behind them, and each Sully AI role runs at 80 to 90% less than the cost of the equivalent human role.
Sully already supports 5,000+ providers and has delivered 50M+ hours of AI work across multiple specialties. See how Sully’s AI workforce removes documentation from the bedside and lets the nurse stay with the patient.
FAQ
Q: What is the correct order for a head-to-toe assessment?
The standard order is top down: general survey and vitals, then head and face, HEENT, neck, chest (heart and lungs), abdomen, extremities, skin, and neurological or musculoskeletal function. The one exception is the abdomen, where you auscultate before palpating so you do not alter bowel sounds. Running the same order every time is what prevents missed findings.
Q: How long does a head-to-toe assessment take?
A routine shift assessment on a stable patient takes about 10 to 15 minutes once you are proficient. A complete admission assessment runs 25 to 30 minutes because it includes full history, medication reconciliation, and detailed system reviews. Expect your first several exams in school or orientation to take longer while you build muscle memory for the sequence.
Q: What equipment do I need for a head-to-toe assessment?
At minimum: stethoscope, penlight, thermometer, blood pressure cuff, pulse oximeter, watch with a second hand, gloves, and hand sanitizer. A full kit adds a reflex hammer, tuning fork, tongue depressor, tape measure, and Snellen chart for vision screening. Most hospitals stock these at the bedside or on the medication cart.
Q: When should a nurse perform a head-to-toe assessment?
Nurses run a head to toe on admission, at the start of every shift, any time the patient’s condition changes, and before and after procedures. In critical care, abbreviated assessments happen every one to two hours. The goal is to set a baseline early so any deviation later in the shift is easy to catch.
Q: Can AI help with head-to-toe assessment documentation?
Yes. AI scribes like Sully.ai’s AI Scribe capture the assessment as you narrate it and populate the EHR in real time, which removes most end-of-shift charting. Sully’s AI Triage Nurse also collects pre-visit symptoms and history, so the head to toe starts with a pre-filled chart. Together they give back one to two hours of direct patient care time per shift.
TABLE OF CONTENTS
Hire your
Medical AI Team
Take a look at our Medical AI Team
AI Receptionist
Manages patient scheduling, communications, and front-desk operations across all channels.
AI Scribe
Documents clinical encounters and maintains accurate EHR/EMR records in real-time.
AI Medical Coder
Assigns and validates medical codes to ensure accurate billing and regulatory compliance.
AI Nurse
Assesses patient urgency and coordinates appropriate care pathways based on clinical needs.