"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="WxV_IOPE7-2309410982-linear-gradient" x1="1" x2="0" y1="0.5951279047551217" y2="0.4048720952448783"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="WwbAIQIz8-2309410982-linear-gradient" x1="0.43478742751482424" x2="0.6358595260107829" y1="0.26" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="ZWsVQcPfn-2309410982-linear-gradient" x1="0.9508213454678907" x2="0.04917865453210929" y1="0" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient><linearGradient id="lTyCGrzzP-2309410982-linear-gradient" x1="0.374937164194436" x2="0.625062835805564" y1="0" y2="1"><stop offset="0" stop-color="rgb(255, 255, 255)"/><stop offset="1" stop-color="rgba(255, 255, 255, 0)"/></linearGradient></defs><g d="M 658.002 1357.705 C 1020.321 1357.705 1314.04 1063.989 1314.04 701.667 C 1314.04 339.347 1020.321 45.626 658.002 45.626 C 295.681 45.626 1.96 339.347 1.96 701.667 L 0 701.667 C 0 338.263 294.598 43.665 658.002 43.665 C 1021.404 43.665 1316 338.263 1316 701.667 C 1316 1065.072 1021.404 1359.672 658.002 1359.672 C 294.598 1359.672 0 1065.072 0 701.667 L 1.96 701.667 C 1.96 1063.989 295.681 1357.705 658.002 1357.705 Z M 658.005 1265.053 C 969.154 1265.053 1221.392 1012.819 1221.392 701.667 C 1221.392 390.517 969.154 138.281 658.005 138.281 C 346.856 138.281 94.619 390.517 94.619 701.667 L 92.659 701.667 C 92.659 389.433 345.77 136.321 658.005 136.321 C 970.241 136.321 1223.352 389.433 1223.352 701.667 C 1223.352 1013.902 970.241 1267.017 658.005 1267.017 C 345.77 1267.017 92.659 1013.902 92.659 701.667 L 94.619 701.667 C 94.619 1012.819 346.856 1265.053 658.005 1265.053 Z M 658.002 1166.116 C 914.513 1166.116 1122.452 958.178 1122.452 701.667 C 1122.452 445.16 914.513 237.22 658.002 237.22 C 401.494 237.22 193.551 445.16 193.551 701.667 L 191.59 701.667 C 191.59 444.077 400.411 235.255 658.002 235.255 C 915.596 235.255 1124.412 444.077 1124.412 701.667 C 1124.412 959.261 915.596 1168.084 658.002 1168.084 C 400.411 1168.084 191.59 959.261 191.59 701.667 L 193.551 701.667 C 193.551 958.178 401.494 1166.116 658.002 1166.116 Z M 281.657 818.28 C 298.572 818.28 314.804 825.001 326.765 836.965 L 458.99 969.182 C 470.582 980.781 486.308 987.298 502.706 987.298 L 612.137 987.298 C 646.284 987.298 673.972 959.61 673.972 925.463 L 673.972 891.504 L 675.939 891.504 L 675.939 925.463 C 675.939 960.7 647.374 989.258 612.137 989.258 L 502.706 989.258 C 485.788 989.258 469.562 982.537 457.599 970.573 L 325.378 838.356 C 313.785 826.757 298.056 820.242 281.657 820.244 L 1.173 820.244 L 1.173 818.28 Z M 746.64 888.714 L 1053.046 888.714 C 1069.967 888.714 1086.194 895.435 1098.16 907.398 L 1259.381 1068.619 L 1257.99 1070.007 L 1096.772 908.79 C 1085.175 897.193 1069.446 890.679 1053.046 890.681 L 746.64 890.681 C 729.724 890.681 713.493 883.957 701.533 871.993 L 685.377 855.845 L 686.769 854.453 L 702.917 870.605 C 714.513 882.201 730.241 888.715 746.64 888.714 Z M 667.685 552 L 512.316 396.894 C 494.66 379.264 484.741 355.356 484.739 330.426 L 484.739 0 L 487.632 0 L 487.632 330.426 C 487.632 354.592 497.248 377.763 514.369 394.851 L 669.739 549.957 Z M 782.851 700.491 C 816.998 700.491 844.686 672.804 844.686 638.655 L 844.686 516.468 C 844.687 499.547 851.409 483.32 863.374 471.355 L 1177.508 157.22 L 1178.896 158.607 L 864.762 472.742 C 853.162 484.337 846.646 500.067 846.646 516.468 L 846.646 638.655 C 846.646 673.89 818.088 702.455 782.851 702.455 L 700.405 702.455 L 700.405 700.491 Z M 130.338 534.223 L 213.07 534.223 C 256.112 534.223 291.003 569.114 291.003 612.156 L 291.003 694.888 C 291.003 711.29 297.514 727.017 309.113 738.611 L 472.887 902.378 L 471.496 903.769 L 307.726 739.995 C 295.761 728.033 289.038 711.807 289.038 694.888 L 289.038 612.156 C 289.038 570.198 255.028 536.188 213.07 536.188 L 130.338 536.188 C 113.419 536.187 97.193 529.465 85.23 517.5 L 77.071 509.345 C 65.107 497.381 58.386 481.153 58.388 464.233 L 58.388 199.526 L 60.348 199.526 L 60.348 464.233 C 60.349 480.631 66.863 496.358 78.458 507.954 L 86.617 516.113 C 98.213 527.709 113.94 534.223 130.338 534.223 Z" fill="transparent" height="1359.6717183844698px" id="DcyumyANr" transform="translate(0 -43.665)" width="1316px"><g opacity="0.5"><path d="M 658.002 1314.039 C 1020.321 1314.039 1314.04 1020.324 1314.04 658.001 C 1314.04 295.681 1020.321 1.961 658.002 1.961 C 295.681 1.961 1.96 295.682 1.96 658.001 L 0 658.001 C 0 294.598 294.598 0 658.002 0 C 1021.404 0 1316 294.598 1316 658.001 C 1316 1021.407 1021.404 1316.007 658.002 1316.007 C 294.598 1316.007 0 1021.407 0 658.001 L 1.96 658.001 C 1.96 1020.324 295.681 1314.039 658.002 1314.039 Z" fill="rgb(255, 255, 255)" height="1316.0065114752902px" id="dxf13D52Y" transform="translate(0 43.665)" width="1316px"/></g><g opacity="0.3"><path d="M 565.347 1128.732 C 876.496 1128.732 1128.733 876.498 1128.733 565.346 C 1128.733 254.196 876.496 1.961 565.347 1.961 C 254.197 1.961 1.961 254.196 1.961 565.346 L 0 565.346 C 0 253.112 253.111 0 565.347 0 C 877.582 0 1130.693 253.112 1130.693 565.346 C 1130.693 877.581 877.582 1130.696 565.347 1130.696 C 253.111 1130.696 0 877.581 0 565.346 L 1.961 565.346 C 1.961 876.498 254.197 1128.732 565.347 1128.732 Z" fill="rgb(255, 255, 255)" height="1130.6960934794101px" id="if1BmYw1S" transform="translate(92.659 136.321)" width="1130.693351805604px"/></g><g opacity="0.15"><path d="M 466.412 930.861 C 722.923 930.861 930.862 722.922 930.862 466.411 C 930.862 209.905 722.923 1.965 466.412 1.965 C 209.904 1.965 1.961 209.905 1.961 466.411 L 0 466.411 C 0 208.822 208.821 0 466.412 0 C 724.006 0 932.822 208.822 932.822 466.411 C 932.822 724.005 724.006 932.828 466.412 932.828 C 208.821 932.828 0 724.005 0 466.411 L 1.961 466.411 C 1.961 722.922 209.904 930.861 466.412 930.861 Z" fill="rgb(255, 255, 255)" height="932.8284667407987px" id="ef75NsYf6" transform="translate(191.59 235.255)" width="932.8219552655086px"/></g><g opacity="0.5"><path d="M 280.484 0 C 297.399 0 313.63 6.721 325.592 18.685 L 457.817 150.902 C 469.408 162.501 485.135 169.018 501.533 169.017 L 610.964 169.017 C 645.111 169.017 672.799 141.33 672.799 107.182 L 672.799 73.223 L 674.766 73.223 L 674.766 107.182 C 674.766 142.42 646.201 170.978 610.964 170.978 L 501.533 170.978 C 484.614 170.978 468.389 164.257 456.426 152.293 L 324.205 20.076 C 312.611 8.477 296.883 1.961 280.484 1.964 L 0 1.964 L 0 0 Z" fill="url(%23cQ4xRdUtr-2309410982-linear-gradient)" height="170.97763275969464px" id="cQ4xRdUtr" transform="translate(1.173 818.28)" width="674.7656780356198px"/></g><g opacity="0.5"><path d="M 61.263 34.261 L 367.669 34.261 C 384.589 34.261 400.817 40.982 412.783 52.945 L 574.004 214.166 L 572.612 215.554 L 411.395 54.337 C 399.798 42.74 384.069 36.226 367.669 36.228 L 61.263 36.228 C 44.347 36.228 28.116 29.504 16.155 17.54 L 0 1.391 L 1.391 0 L 17.54 16.152 C 29.136 27.747 44.864 34.261 61.263 34.261 Z" fill="url(%23WxV_IOPE7-2309410982-linear-gradient)" height="215.55382175474415px" id="WxV_IOPE7" transform="translate(685.377 854.453)" width="574.0036823012563px"/></g><g opacity="0.5"><path d="M 182.946 552 L 27.577 396.894 C 9.921 379.264 0.002 355.356 0 330.426 L 0 0 L 2.893 0 L 2.893 330.426 C 2.893 354.592 12.509 377.763 29.63 394.851 L 185 549.957 Z" fill="url(%23WwbAIQIz8-2309410982-linear-gradient)" height="552px" id="WwbAIQIz8" transform="translate(484.739 0)" width="185px"/></g><g opacity="0.5"><path d="M 82.446 543.271 C 116.593 543.271 144.281 515.583 144.281 481.435 L 144.281 359.248 C 144.282 342.327 151.004 326.1 162.969 314.135 L 477.103 0 L 478.491 1.387 L 164.356 315.522 C 152.757 327.117 146.241 342.846 146.241 359.248 L 146.241 481.435 C 146.241 516.67 117.683 545.235 82.446 545.235 L 0 545.235 L 0 543.271 Z" fill="url(%23ZWsVQcPfn-2309410982-linear-gradient)" height="545.2346136318063px" id="ZWsVQcPfn" transform="translate(700.405 157.22)" width="478.4906210693257px"/></g><g opacity="0.5"><path d="M 71.95 334.696 L 154.682 334.696 C 197.724 334.696 232.616 369.588 232.616 412.63 L 232.616 495.362 C 232.616 511.764 239.126 527.491 250.725 539.084 L 414.5 702.851 L 413.108 704.243 L 249.338 540.469 C 237.373 528.507 230.651 512.281 230.651 495.362 L 230.651 412.63 C 230.651 370.672 196.64 336.661 154.682 336.661 L 71.95 336.661 C 55.031 336.661 38.805 329.939 26.843 317.974 L 18.683 309.819 C 6.719 297.854 -0.001 281.627 0 264.707 L 0 0 L 1.961 0 L 1.961 264.707 C 1.961 281.105 8.475 296.832 20.07 308.428 L 28.229 316.587 C 39.825 328.182 55.552 334.697 71.95 334.696 Z" fill="url(%23lTyCGrzzP-2309410982-linear-gradient)" height="704.2427839655832px" id="lTyCGrzzP" transform="translate(58.388 199.526)" width="414.49961191971533px"/></g></g></svg>)
HPI stands for History of Present Illness. It’s the narrative section of a medical record where a clinician describes the patient’s current health concern in chronological detail, covering eight elements defined by CMS.
If you’ve ever seen “HPI” in a SOAP note, a chart audit, or a billing denial, that’s what it means. The HPI is the story behind the chief complaint, and its depth directly controls the billable level of the visit.
This guide covers what HPI stands for, the eight required elements, how Brief and Extended HPI affect E/M coding, how to write a strong one, and how AI scribes like Sully.ai capture the whole thing automatically.
What HPI Stands For in Medical Records
HPI is short for History of Present Illness. In the UK, the same section is called the History of Presenting Complaint (HPC), but the structure is identical.
The HPI sits right after the chief complaint in a clinical note. The chief complaint is the one-line reason the patient came in. The HPI is the detailed story that follows.
It’s easy to confuse HPI with the rest of a patient’s history. Keep these separate:
Chief Complaint (CC): one-line reason for the visit
HPI: chronological narrative of the current concern
ROS: head-to-toe symptom review
PMH / PFSH: past medical, family, and social history
The CMS 1995 and 1997 Documentation Guidelines are the source of truth for what counts as a compliant HPI. Every auditor, biller, and coder pulls from the same playbook.
The 8 Elements of an HPI
CMS defines eight HPI elements. The number of elements documented is what separates a Brief HPI from an Extended HPI, and it’s the single biggest driver of E/M level on the history side.
Here’s the quick reference.
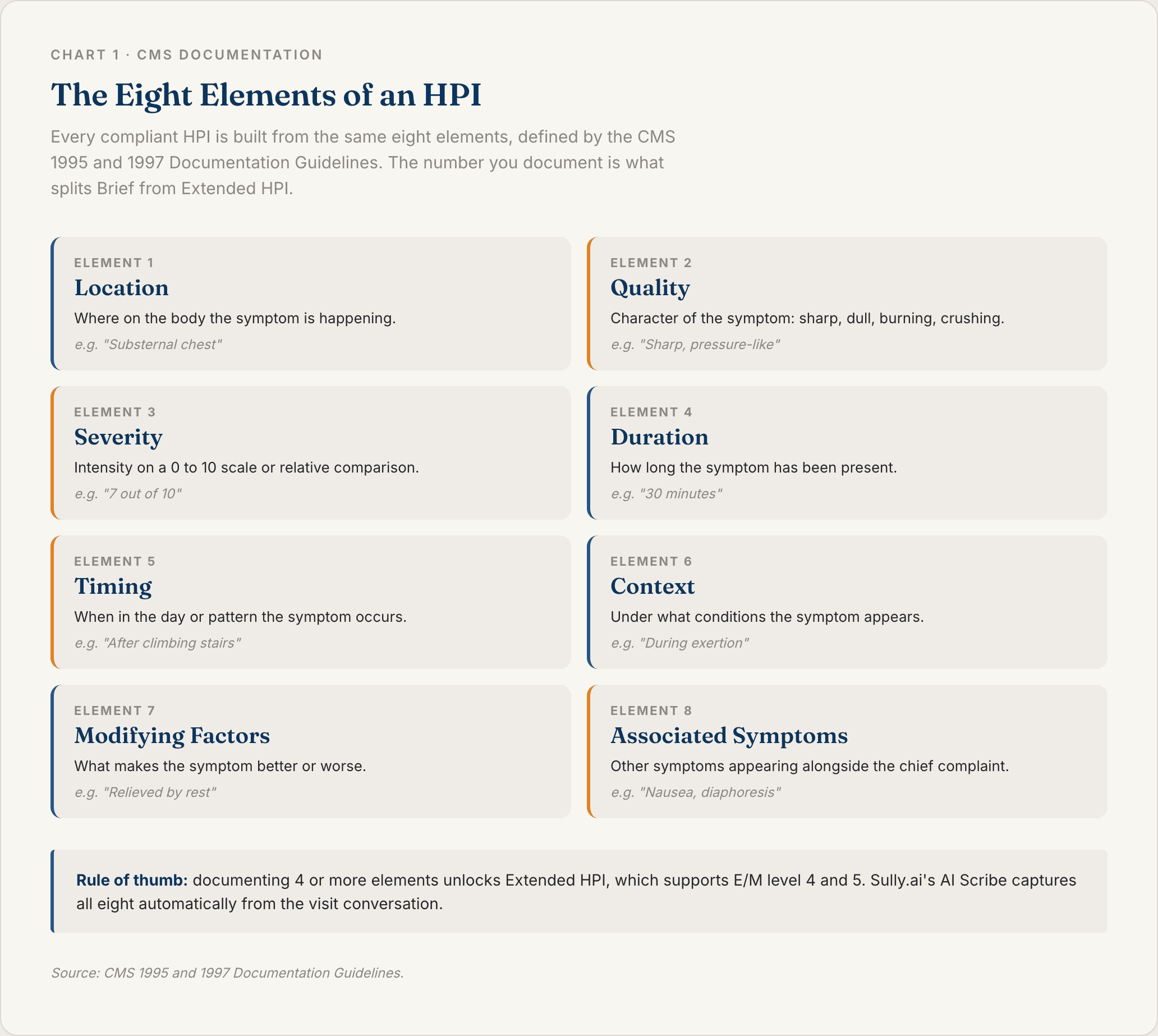
Location
Where on the body the symptom is happening. “Chest pain” is weak. “Substernal chest pain radiating to the left arm” is strong.
Quality
The character of the symptom. Sharp, dull, burning, crushing, throbbing. This is how a patient describes what it feels like.
Severity
A number on a 0–10 scale, or a comparison (“worst headache of my life”). Severity is the element most often missed, and it’s required for an Extended HPI.
Duration
How long the symptom has been present. “Three days” is duration. “Started three days ago” is duration plus onset.
Timing
When during the day or in what pattern the symptom occurs. Morning, nocturnal, post-meal, intermittent every 20 minutes.
Context
What the patient was doing when it started or what situation brings it on. After meals, during exercise, at rest, after medication changes.
Modifying Factors
What makes the symptom better or worse. Rest, ice, NSAIDs, position change, food. This is where clinical reasoning starts to come through.
Associated Signs and Symptoms
What else is showing up at the same time. Nausea with chest pain. Photophobia with headache. Dyspnea with fatigue. These are the clues that move the differential.
Brief HPI vs Extended HPI
CMS splits the HPI into two tiers, and the tier you document caps your E/M level.
Brief HPI: 1 to 3 elements
Extended HPI: 4 or more elements, OR the status of 3 or more chronic or inactive conditions
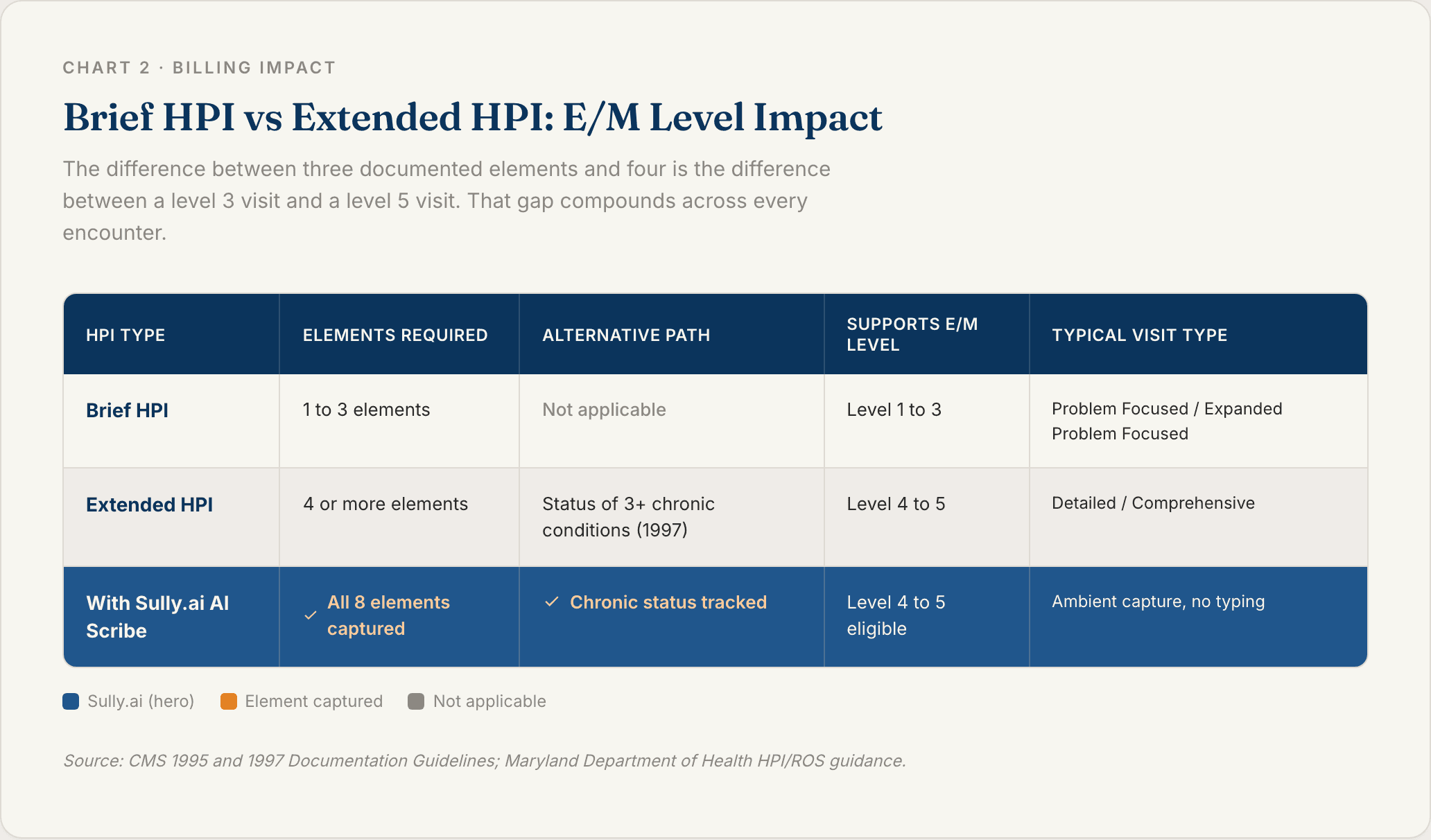
How Brief HPI Affects E/M Level
A Brief HPI caps the visit at Expanded Problem Focused for established patients. That’s an E/M level 3, and the reimbursement difference between a level 3 and a level 4 visit can be 40–60% per encounter.
If you’re documenting three elements when the visit actually warranted five, you’re leaving money on the table every single day.
How Extended HPI Affects E/M Level
An Extended HPI unlocks Detailed and Comprehensive history, which supports E/M level 4 and 5. The 1997 guidelines added an alternative path: documenting the current status of three or more chronic conditions counts as Extended.
That alternative matters for primary care and chronic care management, where patients often come in with a short current complaint but several ongoing problems.
Why HPI Matters for Clinical Documentation
The HPI is doing three jobs at once. It drives diagnosis, it sets the billing level, and it protects you in an audit or a lawsuit.
Impact on Diagnostic Accuracy
The HPI is where the differential gets built. A specific, structured narrative narrows the possibilities before a single test gets ordered.
Vague HPIs push clinicians toward over-testing. Specific HPIs do the opposite. Less imaging, fewer labs, faster answers.
Impact on Billing and E/M Coding
Under-documented HPIs are the number one reason for E/M downcoding on audit. Payers look at the elements, count them, and decide whether the visit level was justified.
A note that describes severity, timing, and modifying factors in one sentence passes. A note that just says “patient reports pain” does not.
Impact on Legal and Audit Defense
In a malpractice case, the HPI is the record of what the patient told you and what you thought about it. A thin HPI is indefensible.
Copy-forward HPIs are worse. If last week’s HPI shows up in this week’s note word-for-word, an auditor will assume the exam never happened.
How to Write a Strong HPI
Two habits separate strong HPIs from weak ones: using a mnemonic and writing in focused narrative.
OLD CARTS and OPQRST Mnemonics
Both mnemonics cover the eight CMS elements with different mental models. Pick the one that sticks.
OLD CARTS | OPQRST |
|---|---|
Onset | Onset |
Location | Provocation / palliation |
Duration | Quality |
Character | Radiation |
Aggravating / alleviating | Severity |
Radiation | Timing |
Timing | |
Severity |
OLD CARTS is more common in primary care and internal medicine. OPQRST is the emergency and EMS standard. Either one works.
Narrative Format and SOAP Integration
The HPI lives in the “S” of a SOAP note. Write it as a paragraph, not a list.
“Mr. K is a 58-year-old with substernal chest pressure that started 30 minutes ago while climbing stairs. Pain is 7/10, dull and squeezing, radiating to the left arm, associated with nausea and diaphoresis. Relieved partially by rest. No prior episodes.”
That’s six elements in four sentences: location, quality, severity, duration, timing, context, modifying factors, associated symptoms. Extended HPI, E/M level 4 or 5 eligible.
Common HPI Documentation Mistakes
Missing severity (the most commonly skipped element)
No timeline or onset
Vague modifying factors (“nothing helps”)
Copy-forward from prior notes
Mixing HPI with ROS (“no fever, no chills, no headache” belongs in ROS)
Fix those five and the quality of your notes lifts immediately.
HPI Documentation Challenges in the EHR Era
HPI quality is falling in most health systems, and the EHR is the main reason.
Time Burden on Physicians
Physicians spend roughly two hours on documentation for every hour of patient care. The HPI is one of the most text-heavy fields in the note, and typing it while talking to a patient is where most of that time goes.
Copy-Forward and Note Bloat
Copy-forward was supposed to save time. It created a second problem: charts full of inaccurate, repeated narratives that don’t reflect the current visit.
Auditors flag copy-forwarded HPIs routinely. Some payers now deny claims when the HPI from consecutive visits is identical.
Template Rigidity and Missed Nuance
Structured templates and dropdowns were supposed to fix note bloat. Instead, they stripped out the narrative thread that makes an HPI clinically useful.
A dropdown for “quality = sharp” loses the patient’s actual words. Words matter in medicine. Templates can’t carry them.
How AI Scribes Automate HPI Documentation
Ambient AI scribes record the visit, extract each HPI element, and write the narrative into the EHR before the physician leaves the room.
Sully.ai is an AI workforce built specifically for healthcare. Sully’s AI Scribe listens to the conversation and produces a full HPI. Sully’s AI Coder reads that HPI and pulls the ICD-10 and CPT codes. The claim goes out clean.
Capturing the 8 HPI Elements Automatically
Sully’s AI Scribe is trained to structure its output around the CMS elements. Location, quality, severity, duration, timing, context, modifying factors, associated symptoms. Every visit, no dropdowns, no templates.
The narrative comes out in the physician’s voice, not in stock template language.
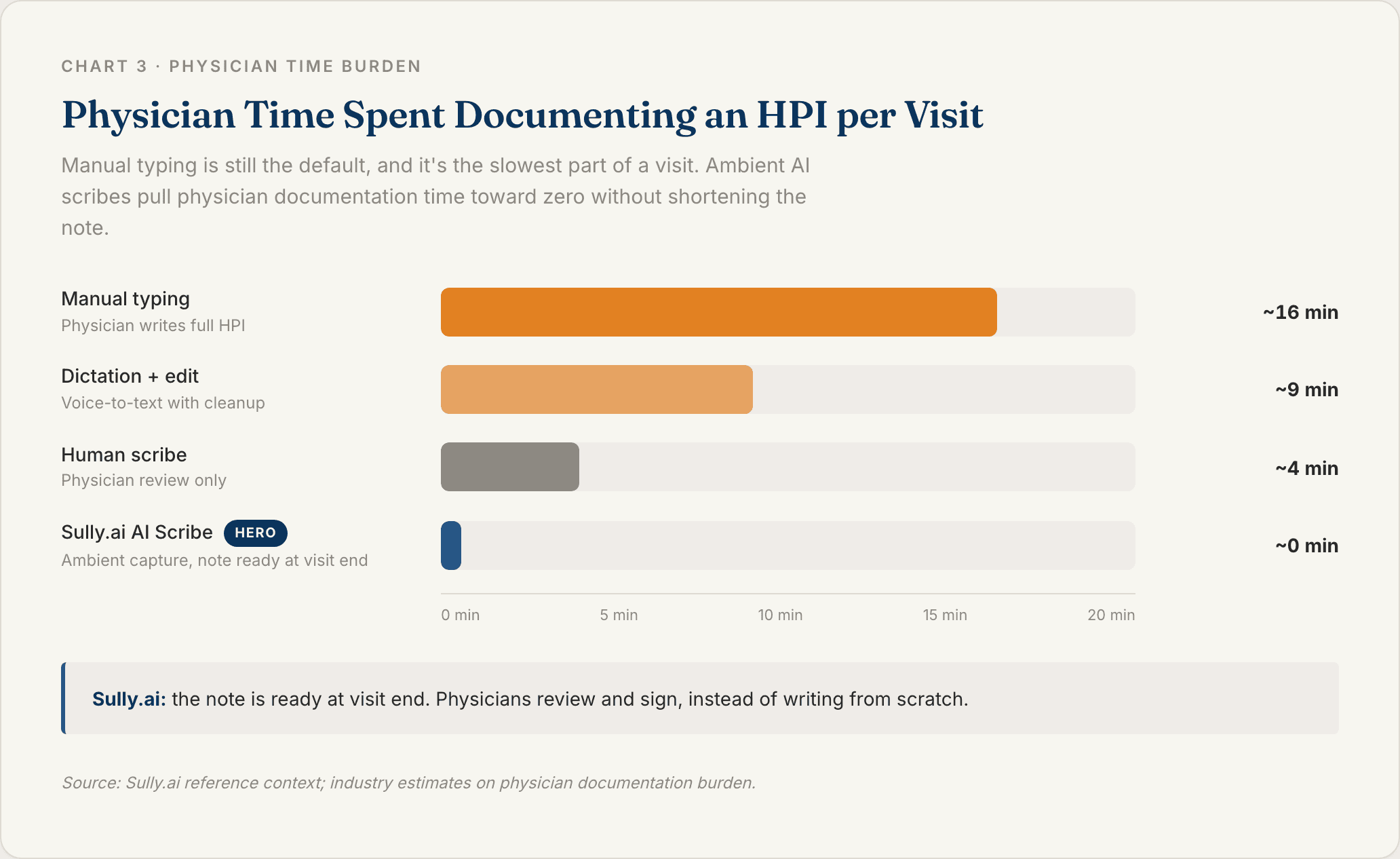
Chart 3: HPI Documentation Time by Method
Connecting HPI to Coding and Billing
This is where most AI scribes stop. Sully does not.
The AI Scribe hands the finished HPI to the AI Coder. The Coder extracts ICD-10 and CPT codes, checks them against payer rules, and submits a clean claim. An Extended HPI gets coded as an Extended HPI, automatically.
That handoff is the difference between a note that exists and a note that gets paid.
Cutting Documentation Time Without Cutting Detail
Sully.ai serves 5,000+ providers and has delivered 50M+ hours of AI work. Each Sully AI role costs 80–90% less than the equivalent human role.
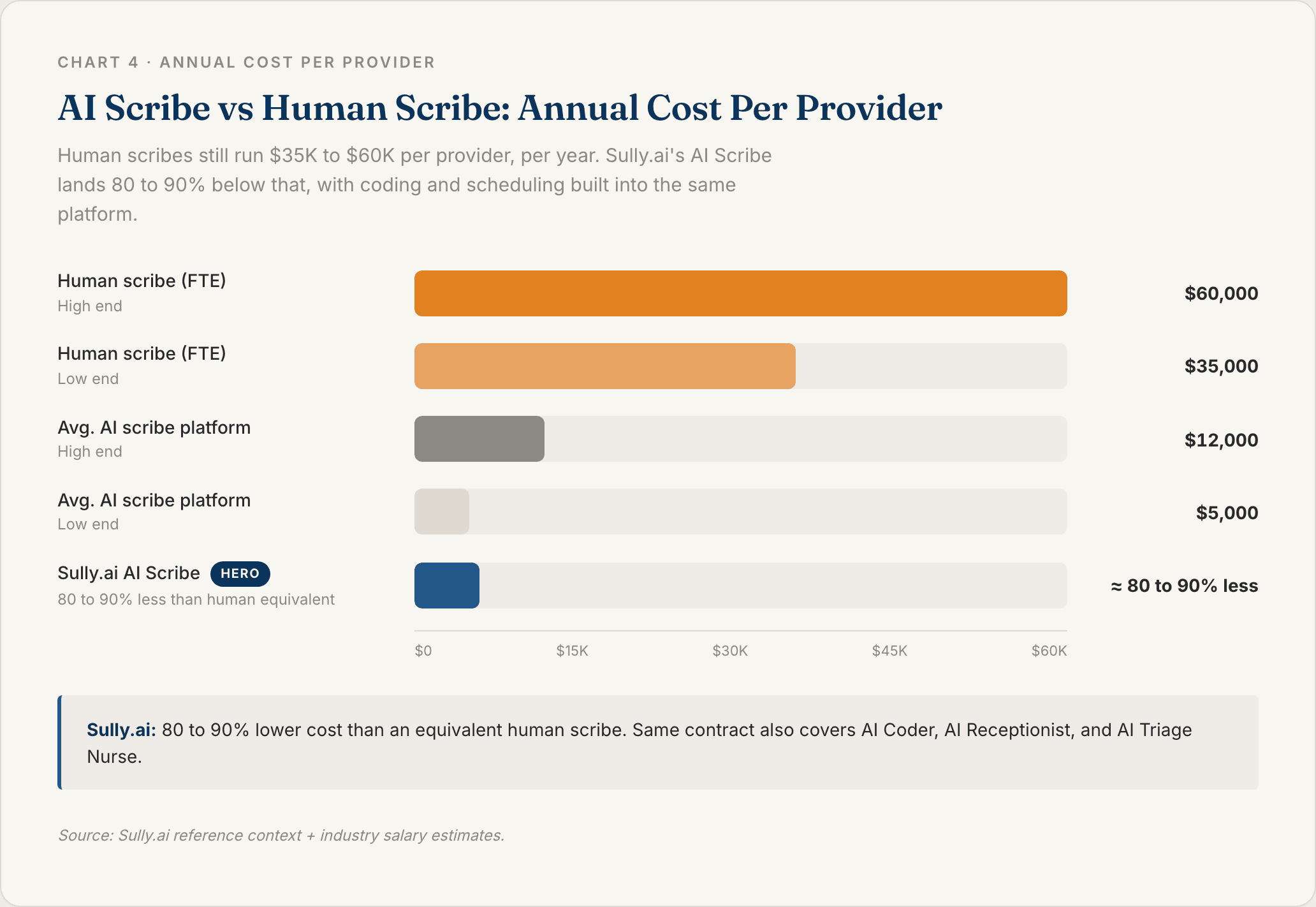
Chart 4: AI Scribe vs Human Scribe Annual Cost
Physicians using Sully reclaim hours per week. HPIs get more detailed, not less. That’s the pattern we see across specialties and EHRs (Epic, Cerner, Meditech, Athenahealth), all through a single integration.
FAQ
Q: What does HPI stand for in medical terms?
HPI stands for History of Present Illness. It’s the section of a medical record that narrates a patient’s current health concern in chronological detail, covering onset, location, quality, severity, timing, context, modifying factors, and associated symptoms. Every E/M visit note includes an HPI, and its depth directly determines the billable visit level. Sully.ai’s AI Scribe captures all eight HPI elements automatically during the patient visit.
Q: What are the 8 elements of an HPI?
The CMS 1995 and 1997 Documentation Guidelines define eight HPI elements: location, quality, severity, duration, timing, context, modifying factors, and associated signs and symptoms. A Brief HPI documents 1 to 3 elements and supports lower E/M levels. An Extended HPI documents 4 or more elements (or the status of 3+ chronic conditions) and supports Detailed or Comprehensive history levels.
Q: What is the difference between HPI and chief complaint?
The chief complaint (CC) is a one-line statement of why the patient came in, for example “chest pain for two hours.” The HPI is the full narrative that develops that complaint across the eight documented elements. Both appear in every E/M note, but the chief complaint is a headline while the HPI is the story.
Q: How long should an HPI be?
There is no minimum word count, but there is a minimum element count. A Brief HPI needs 1 to 3 elements. An Extended HPI needs 4 or more. In practice, well-documented HPIs are 3 to 6 sentences of focused narrative. Length for its own sake does not raise E/M level. Specificity does.
Q: Can AI write an HPI?
Yes. Ambient AI scribes like Sully.ai listen to the patient-physician conversation, identify each of the eight HPI elements, and write a complete narrative directly into the EHR. Sully.ai’s AI Scribe serves 5,000+ providers and cuts documentation time compared to typing HPIs manually or using a human scribe, at 80–90% lower cost than the human equivalent.
TABLE OF CONTENTS
Hire your
Medical AI Team
Take a look at our Medical AI Team
AI Receptionist
Manages patient scheduling, communications, and front-desk operations across all channels.
AI Scribe
Documents clinical encounters and maintains accurate EHR/EMR records in real-time.
AI Medical Coder
Assigns and validates medical codes to ensure accurate billing and regulatory compliance.
AI Nurse
Assesses patient urgency and coordinates appropriate care pathways based on clinical needs.