A continuously evolving benchmark of medical AI performance across clinical reasoning, documentation, and coding tasks.
What We Measure
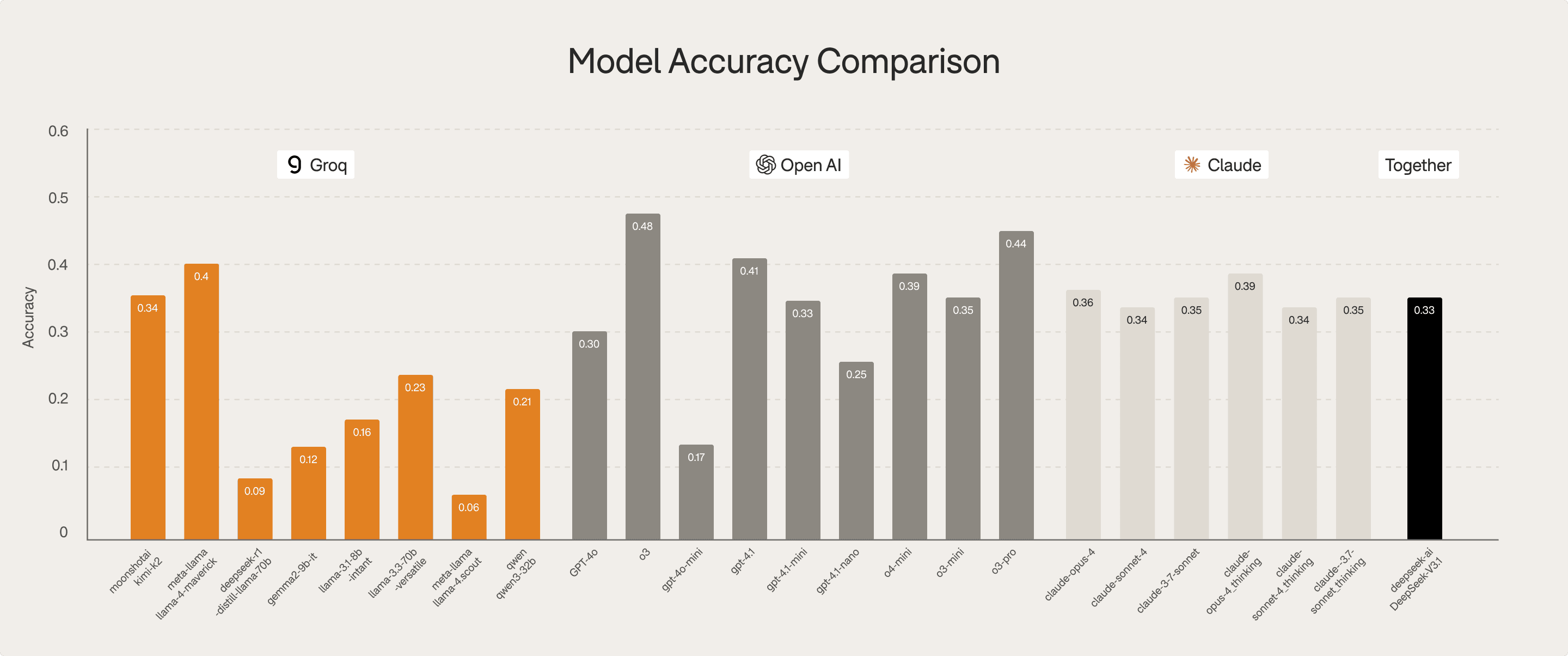
Clinical knowledge accuracy
Diagnostic reasoning strength
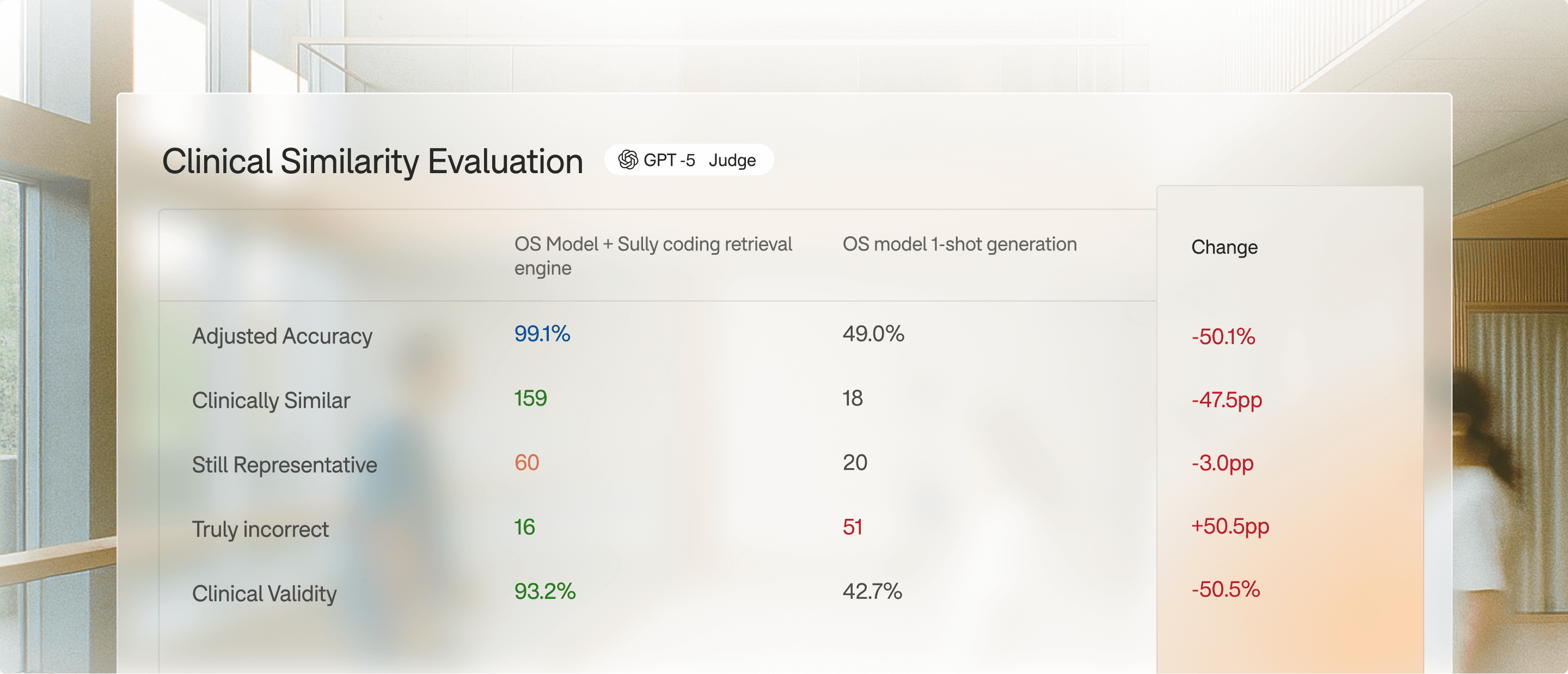
Logical validity and hallucination rates
Safety and guideline adherence
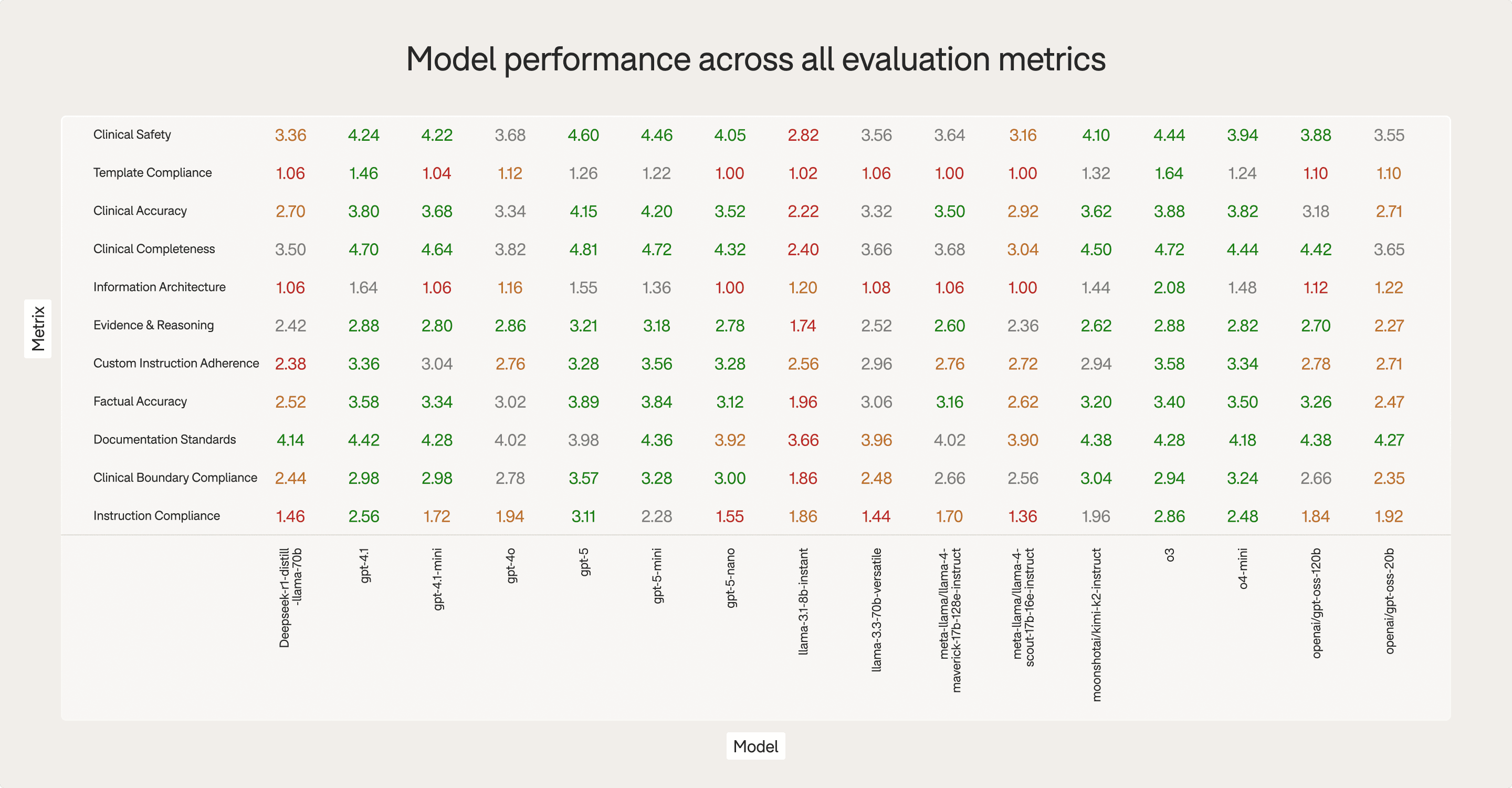
Metrics Assessed
Completeness of medical content
Logical consistency and absence of hallucinations
Clinical validity
Adherence to note structure
Physician usability